Draft domestic homicide review statutory guidance (accessible)
Updated 2 May 2024

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/consultations/updating-the-domestic-homicide-review-statutory-guidance/draft-domestic-homicide-review-statutory-guidance-accessible
Domestic Homicide Review Statutory Guidance
Draft
May 2024
© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at www.gov.uk/government/publications
Any enquiries regarding this publication should be sent to us at [email protected].
Introduction
“Illuminating the past to make the future safer”
Mullane, F. (2017)[footnote 1]
Purpose and legal status
Under section 9(4) of the Domestic Violence, Crime and Victims Act 2004, a Domestic Homicide Review (DHR) is a review of the circumstances in which the death of a person aged 16 or over has, or appears to have, resulted from domestic abuse. Deaths related to domestic abuse are horrendous and pervasive, and still too often hidden from view. A Domestic Homicide Review (DHR) is an opportunity for national and local agencies, local communities, and society as a whole to pay attention to each individual victim and to treat every death as preventable.
It has been over seven years since the DHR statutory guidance was updated in 2016, and over eleven years since the first guidance was published and DHRs were operationalised in 2011. Over this time, we have learnt a great deal about the strengths of DHRs, in addition to where they can be improved to maximise their potential for better understanding and preventing domestic abuse-related deaths. We are dedicated to continuing with the fundamental principles of the DHR, however, we recognise there is room for improvement in the way these are conducted, and the lessons applied.
Since the guidance was last reviewed, the government committed to reforming the DHR process in the 2022 Tackling Domestic Abuse Plan. The reform package included driving systematic change across government, implementing mandatory training for DHR Chairs, enhancing the oversight mechanism for DHRs and refreshing the statutory guidance.
As part of the reform, we plan to amend the legislation that underpins DHRs so that a DHR is commissioned when a death has, or appears to have, resulted from domestic abuse as defined by the Domestic Abuse Act 2021. The 2021 Act introduced a statutory definition of domestic abuse and explicitly including this definition for when a DHR should be considered will ensure that DHRs continue to contribute to our understanding of domestic abuse, and capture learnings to prevent domestic abuse-related deaths.
We are introducing compulsory training for DHR Chairs, to ensure that all DHR Chairs have an in-depth knowledge of domestic abuse and can identify recommendations that will improve the safety of domestic abuse victims and ultimately prevent further deaths.
To improve transparency and contribute to the learning of what can be done differently and ensure better outcomes for potential victims, the Home Office has also launched the Domestic Homicide Review Library which holds all published DHRs. The police and partners now all have easy access to material to learn from previous homicides, and ultimately prevent future homicides.
Structure
The guidance has been broken down into three sections: Section 1: Introduction to Domestic Homicide Reviews; Section 2: Conducting a Domestic Homicide Review; and Section 3:Implementation of Learning – Making the Future Safer. Each chapter provides detailed guidance as to how a DHR should be conducted, outlining the necessary requirements. In addition, to further aid those conducting a DHR, a ‘DHR Toolkit’ has been included at the end of the document to provide templates, examples and signposts to a range of support.
New additions to this revised guidance include a Scoping Review process to improve how early learning is recorded and actioned, this formalises the process of documenting the reasoning why a DHR should or should not be undertaken. Comprehensive information has also been added for conducting DHRs in instances where a domestic abuse victim has died by suicide[footnote 2], neglect or in circumstances that cannot be explained there but there is evidence that they experienced domestic abuse. In addition, this guidance outlines the steps preceding publication of the DHR, including dissemination of learnings and quality assurance. It seeks to map how the DHR process should be conducted to improve how we understand and prevent domestic homicides, and further enhance the reputation of DHRs as world-class domestic abuse-related death reviews.
Furthermore, as the oversight roles of the Domestic Abuse Commissioner (DAC) and Police and Crime Commissioners (PCCs) did not exist when DHRs were created, they have been outlined to improve how national and local learning from DHRs are implemented and monitored.
Audience
This statutory guidance is aimed at those organising, conducting and participating in a DHR. This includes Community Safety Partnerships, the DHR Chair and Panel, the Domestic Abuse Commissioner, Police and Crime Commissioners, organisations working with victims, perpetrators, commissioning services (including the police, local authorities, and the NHS) and the family, friends and community of the victim.
The guidance applies to England and Wales, insofar as it relates to matters in Wales that are reserved to the UK Government – this is primarily policing, and criminal, civil and family justice. In Wales, it is aimed at persons exercising public functions relating to these matters and devolved Welsh authorities must have regard to this guidance in respect to these matters.
It is important to note that in Wales the Welsh Government has introduced the Single Unified Safeguarding Review process, which is conducted where one or more review criteria are met to avoid the need to undertake a series of multiple reviews in relation to the same single incident. For further information on conducting a DHR in Wales please refer to Section 1:3.
All organisations in Wales should refer to the relevant Welsh legislation and associated guidance in respect to devolved matters, such as the Violence Against Women, Domestic Abuse and Sexual Violence (Wales) Act 2015 (‘the 2015 Act’) and its associated guidance.
We expect those carrying out devolved and non-devolved functions to continue to work together to implement the purposes of both the 2015 Act and the 2021 Act where relevant and appropriate.
To develop this Domestic Homicide Review Statutory Guidance, a range of statutory, specialist and voluntary organisations and individuals have been consulted and we thank them for their contributions.
Section 1: Introduction to Domestic Homicide Reviews
1. Purpose of a DHR
The purpose of a DHR is to understand what lessons can be learnt from domestic abuse-related deaths and to identify and implement local and national learning to better safeguard victims of domestic abuse.
DHRs are not inquiries into how the victim died or into who is culpable; that is a matter for coroners and criminal courts, respectively, to determine as appropriate. DHRs are not specifically part of any disciplinary inquiry or process. However, the coroner’s inquest and police investigation will be of considerable assistance as a DHR may review these and in some cases identify evidence of domestic abuse that had not been recognised in other processes.
Local learning: A DHR should establish what lessons are to be learnt from the death. Specifically, the way in which local professionals and agencies work – and work together – to identify and safeguard victims. In addition to professionals, agencies and multi-agency responses, families, friends, neighbours and colleagues are those involved in a coordinated community response, therefore their insight can be utilised to inform the DHR and any local learning. Our communities play a key role alongside professional organisations to identify barriers faced when attempting to access services, gaps in local service provision and determine how these can be addressed with changes to local processes and systems. This learning should inform the local response to tackling domestic abuse.
National learning: While DHRs are rooted in the local area, it is likely that the process will identify learnings which are applicable nationally. Where gaps are identified that need to be addressed at a national level, these should be addressed to the relevant Government department and organisational body (for example, NHS England and the College of Policing) with an appropriate recommendation.
To achieve their purpose, a DHR must be victim-centred and conducted in a trauma-informed way. A DHR should aim to see life through the eyes of the victim and their children. To achieve this, the DHR Chair must work with the people the victim was close to, family, friends, neighbours, community members, colleagues and professionals. This will help reviewers to understand the victim’s reality; to identify any barriers the victim faced and learning why any interventions did not work to keep them alive. The key to a victim-centred DHR is situating the review in the home, family and community of the victim. Whilst a DHR should remain victim-centred, they should consider engaging with perpetrators to help the panel understand the full range of challenges facing the victim, and to identify if there were opportunities to prevent the perpetrator from engaging in abuse.
2. Criteria and definitions for a DHR
Under section 9(1) of the Domestic Violence, Crime and Victims Act 2004, a Domestic Homicide Review is a review of the circumstances in which the death of a person aged 16 or over has, or appears to have, resulted from domestic abuse.[footnote 3] It is held with a view to identifying the lessons to be learnt from the death.
Where the definition set out in paragraph 2.1 has been met, then a Domestic Homicide Review should be undertaken.
3. Conducting a DHR in Wales: The Single Unified Safeguarding Review (SUSR)
What is a Single Unified Safeguarding Review (SUSR)?
The Single Unified Safeguarding Review (SUSR) is a single review process incorporating all homicide reviews in Wales. It is essential that organisations and agencies that work in Wales and across both Wales and England follow the SUSR Statutory Guidance to effectively collaborate with SUSRs. This ensures that relevant lessons are learnt across the governance structures and required changes and adjustments are made where appropriate locally, regionally, and nationally.
The SUSR partnership approach underpins the innovative work at strategic and operational levels in Wales. The approach ensures partners and organisations work together across disciplines and partnership arrangements in Wales, to share learning and prevent harm. Organisations such as the Welsh Government, Public Health Wales, local authorities, local health boards, His Majesty’s Prison and Probation Service, Policing in Wales (Chief Constables and Police and Crime Commissioners) and the third sector work should work together across Community Safety Partnerships, Regional Safeguarding Boards and Public Service Boards to ensure learning (individual and thematic) is shared effectively and acted on appropriately, to protect people and communities from harm.
The Government of Wales Act 1998 (GoWA 1998) provided for the transfer of executive functions from UK Government Ministers to the National Assembly for Wales (now Senedd Cymru). Under GoWA 2006, those functions were transferred from the National Assembly for Wales to the Welsh Ministers. Welsh Ministers now exercise the majority of the executive and subordinate legislative powers in relation to local government, despite whether those powers are conferred by an Act of Senedd Cymru or an Act of the UK Parliament. Section 108A of and Schedules 7A and 7B of GoWA 2006 establish the basis of the legislative competence of the Senedd to make primary legislation. Schedule 7A specifies the areas of policy in respect of which only Parliament can legislate. Any area not listed within Schedule 7A is within the legislative competence of the Senedd; Schedule 7B contains general restrictions on the way in which the Senedd may exercise its legislative competence.
Services such as education, health, housing, local government, social welfare and Fire and Rescue are within the legislative competence of the Senedd Cymru. Therefore, all reviews undertaken in Wales, must be compatible with the devolution settlement and relevant processes established in Wales. To ensure learning is embedded in policies and processes, where possible, the relevant Welsh Ministers should be made aware of review recommendations which sit within their policy portfolios.
Overarching Purpose of Single Unified Safeguarding Review
The Single Unified Safeguarding Review seeks to develop a single, proportionate mechanism in which to conduct a review following the most serious of incidents in Wales. Where one or more review criteria are met, to avoid duplication, the Single Unified Safeguarding Review process will avoid the need to undertake a series of multiple reviews on single incidents. These include Domestic Homicide Reviews, Child Practice Reviews, Adult Practice Reviews, Mental Health Homicide Reviews and Offensive Weapons Homicide Reviews.
The Single Unified Safeguarding Review process has been created to:
- deliver a single review instead of multiple reviews in relation to an incident(s);
- create a simplified yet concentrated approach to reviews which reduces trauma to families and ensures the victim/family impacted is at the heart of the review process;
- take a “one public service” approach so that victims and families are not left to make sense of the work of different professions or agencies;
- eliminate duplication of effort to ensure the most efficient utilisation of resources and achieve best value;
- produce a Review Report that is focussed on improving service delivery with a clear Action Plan that will be used by the Single Unified Safeguarding Review Co-ordination Hub, Regional Safeguarding Boards, Community Safety Partnerships and other relevant groups to ensure that recommendations are implemented; and
- enable the sharing of information, recommendations, and thematic learning to safeguard future generations utilising the Wales Safeguarding Repository to improve practices and prevent future harm.
What does this mean for DHRs undertaken in Wales?
The definition and criteria for DHRs are replicated in the SUSR Statutory Guidance. Therefore, if the incident meets the criteria for a DHRs in Wales the SUSR process should be instigated. It should be noted that there are some additional steps that need to be undertaken to ensure the DHR legislative requirements are met for reviews in Wales. These are stipulated in the SUSR process and include the submission of the final review to the Home Office Quality Assurance Panel and to the Office of the Domestic Abuse Commissioner.
A link to the Single Unified Safeguarding Review Statutory Guidance will be provided once available.
Section 1 of The Domestic Abuse Act 2021 defines domestic abuse as:
(2)Behaviour of a person (“A”) towards another person (“B”) is “domestic abuse” if—
(a) A and B are each aged 16 or over and are personally connected to each other, and
(b) the behaviour is abusive.
(3) Behaviour is “abusive” if it consists of any of the following—
(a) physical or sexual abuse;
(b) violent or threatening behaviour;
(c) controlling or coercive behaviour;
(d) economic abuse (see subsection (4));
(e) psychological, emotional or other abuse; and it does not matter whether the behaviour consists of a single incident or a course of conduct.
(4) “Economic abuse” means any behaviour that has a substantial adverse effect on B’s ability to—
(a) acquire, use or maintain money or other property, or
(b) obtain goods or services.
(5) For the purposes of this Act A’s behaviour may be behaviour “towards” B despite the fact that it consists of conduct directed at another person (for example, B’s child).
(6) References in this Act to being abusive towards another person are to be read in accordance with this section.
(7) For the meaning of “personally connected”, see section 2.
Section 2 of The Domestic Abuse Act 2021 defines “personally connected” as:
(1) For the purposes of this Act, two people are “personally connected” to each other if any of the following applies—
(a) they are, or have been, married to each other;
(b) they are, or have been, civil partners of each other;
(c) they have agreed to marry one another (whether or not the agreement has been terminated);
(d) they have entered into a civil partnership agreement (whether or not the agreement has been terminated);
(e) they are, or have been, in an intimate personal relationship with each other;
(f) they each have, or there has been a time when they each have had, a parental relationship in relation to the same child (see subsection (2));
(g) they are relatives.
(2) For the purposes of subsection (1)(f) a person has a parental relationship in relation to a child if—
(a) the person is a parent of the child, or
(b) the person has parental responsibility for the child.
(3) In this section—
“child” means a person under the age of 18 years;
“civil partnership agreement” has the meaning given by section 73 of the Civil Partnership Act 2004;
“parental responsibility” has the same meaning as in the Children Act 1989 (see section 3 of that Act);
“relative” has the meaning given by section 63(1) of the Family Law Act 1996.
When a victim of domestic abuse dies by suicide, from neglect or in unexplained circumstances, a DHR must be considered. Due to the possible number of cases that will meet these criteria we do not anticipate it will be possible for every case to progress to a DHR. However, the initial Scoping Review will ensure that learning is taken from every case. For more information on Scoping Reviews, please see Section 2:4.
Factors to consider when commissioning a DHR:
- Multiple incidents of domestic abuse reported to the police and/or other agencies and/or specialist organisations (e.g. GP, domestic abuse charities, school)
- Early indication of possible important learning, for example:
- reported or anecdotal evidence from family and friends of controlling or coercive behaviour;
- the victim had no recourse to public funds or was on a spousal visa;
- the victim was being managed by, or should have been referred to, a Multi-Agency Risk Assessment Conference (MARAC) or another multi-agency forum;
- the victim had no prior contact with any relevant agencies;
- or the victim had multiple disadvantages (multiple disadvantages refers to those people who face multiple and intersecting inequalities including protected characteristics[footnote 4], experience of crimes that fall under the banner of violence against women and girls (VAWG), substance use, mental ill health, disabilities, homelessness, being involved in the criminal justice system and the removal and fear of removal of children).
A DHR is not a criminal investigation. Therefore, there is no expectation that it will attempt to prove that a domestic abuse victim’s death was directly a result of domestic abuse. However, the DHR should highlight the learning that can be taken from the actions taken (or not taken) by those who could and/or should have treated any potential domestic abuse present as a risk to be managed.
A DHR needs to establish both a victim and perpetrator(s) of domestic abuse. Therefore, the Community Safety Partnership (CSP) need to be confident that a review can be commissioned on that basis. However, as a DHR is not a criminal investigation, if a perpetrator is not identified by law enforcement agencies, it is not the responsibility of the review to do so and should not prevent the DHR from going forward.
Section 2: Conducting a Domestic Homicide Review
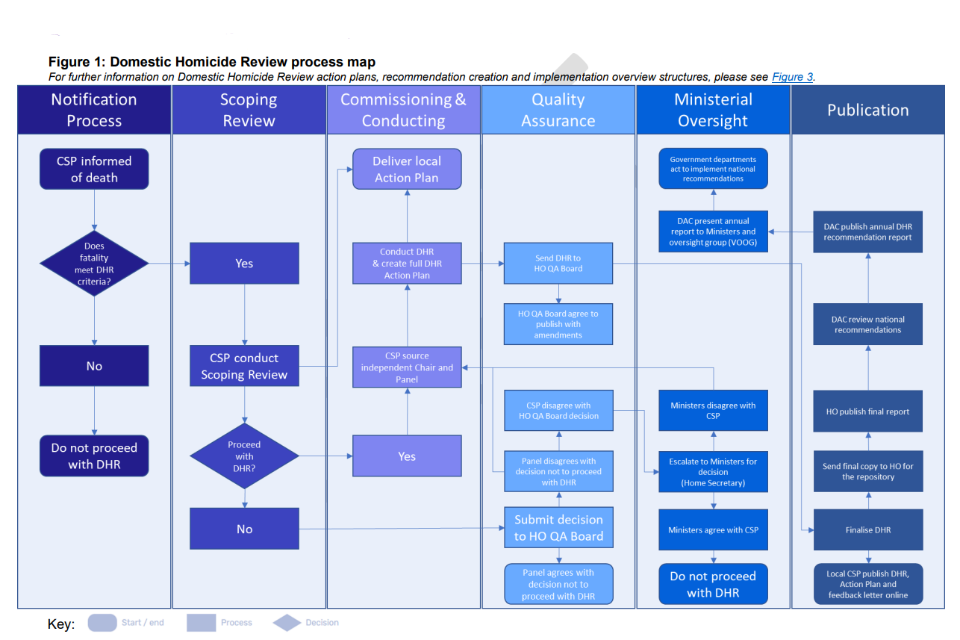
Figure 1: Domestic Homicide Review process map For further information on Domestic Homicide Review action plans, recommendation creation and implementation overview structures, please see Figure 3.
4. Notification of a death to the Community Safety Partnership
The Community Safety Partnership (CSP) should be notified of a domestic abuse-related death by the local area police force. As stated in section 9(3) of the Domestic Violence, Crime and Victims Act 2004, any person or body required to establish or participate in a DHR must have regard to any guidance issued by the Secretary of State as to the establishment and conduct of DHRs.
Whilst notifications are typically made by the local area police force, if relevant persons, bodies, friends or family members of an individual, become aware of the qualifying circumstances of a death, or if they become aware of such facts that make it likely the conditions in section 9 of the 2004 Act are satisfied in relation to a death, a notification can be made to the local CSP directly.
Efforts should be made to contact the CSP via email or in writing, so information is dated and documented. A friend or family member may find it useful to contact a statutory agency or specialist support service who had contact with the deceased individual for support when contacting the CSP.
5. Scoping Review process
A CSP must conduct a Scoping Review for all fatal incidents that meet the criteria for a DHR within four weeks of notification. The Scoping Review can be a desk-based exercise or the CSP may choose to convene a panel or utilise existing decision-making structures. The purpose of the Scoping Review process is to:
- assess whether a full DHR is needed (Scoping Reviews should not replace the DHR process);
- act as a scoping tool to determine the proportionality of the review required;
- determine whether a DHR is the most appropriate form of review (see section 8 on parallel reviews for more information); and
- ensure early learnings from the death are recorded and acted upon swiftly.
The CSP should notify the family of the victim that a Scoping Review is being undertaken. The process should be explained and their views on whether they think a DHR should be commissioned should be sought. This engagement must be managed sensitively and independent specialist advocacy must be offered to the family at the earliest opportunity.
The Scoping Review process can support the CSP to determine whether a death falls in scope of multiple reviews. More detail about conducting parallel investigations can be found in Section 2:7. The Scoping Review process can also help to ascertain if there are any ongoing criminal proceedings which the DHR Chair will need to be aware of. Further information about managing DHRs in these instances can be found in Section 7.
5a. Conducting the Scoping Review Process
The Scoping Review template can be found in Annex C. A Scoping Review must include:
- a short summary of events that led up to the death and short summary of agency interaction (if any) with the victim and perpetrator;
- key emerging learning and themes;
- an action plan;
- whether a DHR will be commissioned and a rationale to support decisions not to commission a DHR; and
- whether a DHR will be commissioned but must be paused due to ongoing criminal proceedings. See Section 9 for more information.
Following a Scoping Review, the CSP are responsible for deciding whether to proceed with a DHR Review. Any early findings, emerging themes or action plans should be addressed in the subsequent DHR. The Scoping Review, including where a decision not to proceed with a DHR must then be sent to:
- the Home Office DHR team on [email protected];
- the Domestic Abuse Commissioner on [email protected]; and
- the Local Police and Crime Commissioner.
5b. Decisions not to conduct a DHR
When the CSP make the decision not to proceed with a DHR the independent Home Office Quality Assurance (QA) Board[footnote 5] will review Scoping Reviews where the CSP has decided not to conduct a DHR. The CSP will be notified within four weeks if the QA Board agree with the decision or if they recommend conducting a DHR.
If the CSP disagrees with the QA Board’s recommendation to conduct a DHR, the decision will be escalated to the Home Secretary who will make the final decision. The Home Secretary has the power to direct a CSP to undertake a DHR where deemed appropriate.
6. Coordinating a Domestic Homicide Review at the local level
Once a Scoping Review has been completed and the decision to proceed with a DHR has been made, the CSP should formally commission a DHR.
6a. Convening a DHR Panel
When a decision is made to undertake a DHR, the CSP must establish a local DHR Panel. The Panel must bring relevant expertise to the fore and ensure that the dynamics and circumstances of the death are seen through multiple and relevant lenses, such as professional and specialist voluntary services, family and friends, emergency response teams and the victim.
The DHR Panel must include individuals from the statutory agencies listed under section 9(4) of the Domestic Violence, Crime and Victims Act 2004. It must also include representation from the national or local VAWG[footnote 6] specialist sector[footnote 7], and where appropriate expert representatives on marginalised groups who will have knowledge on the dynamics of domestic abuse, how it manifests and represent the perspective of the victim and/or, where appropriate, the perpetrator.
Panel members must be independent of any line management of staff involved in the case. They must also be sufficiently senior to have the authority to commit to decisions made on behalf of their agency during a panel meeting and demonstrate how they will ensure learning is embedded within their organisation.
Expectations of Panel engagement throughout the DHR:
-
Panel members should be able to consistently attend DHR meetings.
-
In addition to regular meetings, the Panel must hold an initial meeting to agree the scope and terms of reference for the DHR, a meeting on Individual Management Reviews and a final meeting to discuss the final draft of the DHR. We encourage the Panel to meet quarterly to receive updates from the DHR Chair and provide feedback and constructive challenge throughout the process.
-
The Panel should consider themselves as co-producers of the DHR. As such, they should seek to engage in the process of creating the Terms of Reference scrutinising information that is collated to identify learnings and participate in developing the final DHR.
-
DHR Panel members should use their expertise to consider and constructively challenge the DHR Chair and the interim findings to ensure it comprehensively considers all relevant issues. Debate is encouraged however any disagreements between DHR Panel members must be resolved by the members and DHR Chair. If they cannot be resolved, the DHR will need to record the areas of disagreement and actions taken towards a resolution. The Home Office will not arbitrate when there is disagreement amongst Panel members.
The CSP must have local governance structures in place to monitor the implementation of the DHR’s action plan. The CSP should ensure the DHR Panel are aware of these and their responsibilities within them.
6b. Appointing a Chair for the DHR
The CSP is responsible for appointing an independent Chair of the local DHR Panel. To ensure independence the CSP must review if they are repeatedly chairing within the same area, whether they have connections to any panel members or organisations represented, personal or professional. The DHR Chair should not be directly associated with any agencies involved in the DHR or the CSP. If a DHR Chair was previously a member of one of the agencies associated with the DHR or the CSP or a neighbouring area, it should be made clear how much time has elapsed since they left that agency. An ‘independence statement’ should be included as an appendix to the DHR, setting out the Chair’s career history, independence and any conflicts of interests. The Chair must have completed the Home Office DHR Chair’s training.[footnote 8]
The DHR Chair is responsible for managing the DHR process and ensuring all avenues that may provide learnings to prevent future domestic abuse-related deaths are explored.
The DHR Chair is also responsible for producing, ensuring quality and compliance of the final DHR, based on evidence that DHR Panel decides is relevant. The Chair is required to use the DHR Template provided in Annex A. A final version of the DHR and accompanying DHR Schema should be sent to the CSP for local governance approvals and then sent to the Home Office. A copy of the DHR Data Capture Form is included as Annex G.
Any individual which the CSP seeks to appoint as DHR Chair must have completed the Home Office DHR Chair’s training. The purpose of this is to ensure DHR Chairs can conduct a DHR effectively, successfully identify all relevant learning and develop recommendations that will improve the safety of domestic abuse victims and prevent further deaths.
CSPs should consider the skills and expertise of any individuals they are seeking to appoint as a DHR Chair. Alongside completion of Home Office Chair’s training, the CSP should be confident the DHR Chair has the following:
- expert knowledge of domestic abuse policy, including research, guidance and legislation relating to adults and children, including for example the Domestic Abuse Act 2021, Domestic Abuse Act Statutory Guidance (2022), Controlling or Coercive Behaviour Statutory Guidance Framework (2023), Serious Crime Act 2015, Children’s Act 2004, the Care Act 2014 and the Equality Act 2010;
- understanding and experience in trauma-informed practices;
- clear understanding of the nature of confidentiality;
- understanding of each individual’s personal experiences and needs and its impact on an individual’s experiences and interactions with agencies; an understanding of the role and context of the main agencies likely to be involved in a DHR;
- experience in managing multiple stakeholders;
- ability to draw multiple strands of complex information together and produce a strategic assessment;
- good written and verbal communication skills;
- experience of writing formal reports, preferable but not essential;
- an understanding of wider statutory review frameworks such as child or adult reviews; and
- experience of supporting domestic abuse victims or frontline experience in the domestic abuse sector is favourable although not essential.
7. Conducting the Domestic Homicide Review
In consultation with the DHR Panel, the DHR Chair should determine the scope of the DHR and create a Terms of Reference. The Terms of Reference should be drafted by the DHR Chair and must be shared with the DHR Panel for comment and agreement. In addition, the Terms of Reference should be shared with family and friends if they are engaging in the DHR. These may need to be revisited as the DHR progresses and as new information emerges. Any reconsideration or changes to these documents will need to be agreed by the DHR Panel.
If a DHR is anticipated to run in parallel to a criminal investigation or prosecution, the DHR Chair should inform the police. This will allow the police the opportunity to express their views and input to the DHR Terms of Reference before they are finalised.
7a. Scope of the DHR and Terms of Reference
A non-exhaustive list of factors that the DHR Chair should consider when developing the scope of the DHR includes:
-
The time periods under review in the lives of the victims and perpetrators. Whilst it may not be possible to determine a cut-off point as to how far back the DHR should go, efforts should be made to learn about their history to help better understand the events leading to the death.
-
The agencies that had been involved with the victim or perpetrators should be asked to contribute an Individual Management Review (IMR). The DHR Chair should also consider contacting agencies that have not come into contact with the victim or perpetrator, but might have been expected to do so. This could support the development of learning that improves understanding of why contact was not made.
-
A determination of whether the victim or perpetrator were subject to Multi-Agency Risk Assessment Conference (MARAC) or Multi-Agency Public Protection Arrangements (MAPPA) or other arrangements. The DHR Chair should seek to request the minutes or Memorandum of Understandings from these meetings.
-
The terms of engagement with family members, friends and other support networks (for example, co-workers and employers, neighbours etc); and where appropriate, the perpetrator, should be clarified by the DHR Chair. Consideration should be given to how family members, friends and support networks of the victim will be engaged and updated and how the services of an independent advocate can be utilised. Arrangements for giving feedback and sharing the contents of the DHR with family members/next of kin before publication should also be clarified.
-
Consideration by the DHR Chair of how any public and media attention and engagement should be managed before, during and after the DHR, and work with the CSP who are responsible for this.
-
Specific considerations around equality and diversity issues relating to the victim and perpetrator should be explored, these include: age, disability (including learning disabilities), gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion and belief, sex and sexual orientation. Further information regarding diversity and inclusion can be found in Section 2:11.
-
Consideration of other reviews taking place into the case, including decisions to conduct joint or parallel reviews. The Terms of Reference should ensure the key requirements of both processes are clearly identified and met. Further information can be found in Section 8.
-
Establish whether there have been other DHRs in the same local authority area. If so, consider whether there are relevant recommendations to consider alongside the current DHR’s learning.
It is critical that there is control over any information which is shared, to ensure information does not jeopardise or undermine the criminal investigation or other criminal justice proceedings running in parallel to the DHR. It may be necessary to wait for the resolution of criminal investigations and proceedings before certain details are shared with DHR Panel members or included in the DHR. This should be balanced against the benefits of learning being identified in a timely manner and action taken, which may help individuals avoid becoming victims or perpetrators of homicide in the future. Further information about conducting a DHR alongside a criminal investigation can be found in Section 2:8.
The DHR Chair should agree with the CSP any plans for briefing sessions or learning events for relevant review partners and appropriate bodies to establish what lessons are to be learnt from the incident. The learnings may also be circulated to relevant partners.
7b. Additional evidence and research
At this stage the DHR Chair must consider what additional evidence, information or research the DHR would benefit from. Any findings, analysis or recommendations from the DHR should be evidence based. Therefore, at a minimum the following should be included:
-
Individual Management Reviews (IMR):
- IMRs should allow agencies to look openly and critically at individual and organisational practices and the context within which professionals were working (culture, leadership, supervision, training, etc.), to see whether the death indicates that gaps exist, or practice needs to be changed or improved to support professionals to carry out their work to the highest standards;
- identify interactions with the victim and / or perpetrator;
- identify how and when those changes or improvements to practice will be implemented;
- identify examples of good practice within agencies;
- and the DHR Chair is expected to invite IMR authors to present and discuss drafts during DHR Panel meetings. The template for IMR is included as Annex D.
-
Interviews with family, friends and communities to ensure the DHR presents a comprehensive picture of the victim and their life. These can be:
- interviews with the victim’s family and friends;
- interviews with the perpetrators family and friends;
- and consider approaching the victim and perpetrator’s employers where relevant.
-
Secondary research and evidence to support findings and recommendations. Where research is used, DHR Chair’s must ensure it is relevant to the case. This can include:
- immediate actions already taken;
- actions identified in the Scoping Review;
- reference to previous DHR’s in the local area;
- submissions or reports on existing strategic assessments from agencies, the CSP or other relevant bodies about their response to domestic abuse;
- and published research.
8. Compiling the Domestic Homicide Review
The analysis of information is a crucial component of the DHR. The DHR Chair and panel must probe the evidence provided and examine how and why the death occurred. The analysis must consider whether different decisions or action could have led to a different course of events. It is also an opportunity to highlight where good practice occurs.
Once the Terms of Reference are finalised, the evidence has been considered and agreed by the DHR Panel, and the panel have engaged with family and friends, the DHR Chair should draft the DHR using the DHR Template included as Annex A. A non-exhaustive list of items to consider whilst drafting the DHR are outlined below:
-
Review all information collated during the Scoping Review, IMRs submitted by agencies and interviews, and summarise the information in a combined chronology leading up to the incident.
-
Analyse the information gathered to identify key learning and recommendations. It may be necessary to prioritise what issues are the most important to address when identifying the learning from the incident.
-
Ensure data collection from all relevant sources is documented to enable the DHR Schema to be populated. The document should be sent alongside the final DHR to the Home Office on completion. A template for the Schema is included as Annex G.
-
The CSP must complete the DHR local Action Plan (a template has been provided in Annex B). Arrangements for the oversight of the implementation of the Action Plan should also be made clear in the template. Further guidance on recommendations and oversight can found in Figure 3.
8a. Trauma-Informed Approach
Conducting a DHR requires a trauma-informed approach[footnote 9],[footnote 10]. A DHR will engage with significant trauma, including the trauma suffered by the victim of the DHR, the family, friends and community of the victim and the perpetrator, in addition to the potential secondary trauma experienced by panel members. How the DHR will take a trauma-informed approach must be established at the first panel meeting.
Using a trauma-informed approach when conducting a DHR will not only act to prevent further re-traumatisation of the family, friends, community of the victim and the perpetrator and panel members; it will also allow the DHR to collectively understand and acknowledge the impact of the past trauma experienced by the victim. By understanding these experiences, the Panel will be able to identify the relevance of how a victim may have perceived or responded to certain actions or circumstances (e.g. childhood trauma can impact the child or young person’s thinking about their social world, potentially leading to social isolation, low self-esteem, and mistrust of others, which in turn can have implications for how the child or young person engages with a professional[footnote 11]). This highlights that an individual’s engagement with services is impacted by the multi-dimensional experiences of trauma, therefore service provisions should reflect this by using a ‘multipronged approach’ to meet their needs and effectively intervene and improve the outcomes for potential victims and perpetrators.
To do this successfully the DHR Chair and Panel should work to increase practitioners’ awareness of the individual and community impact of trauma. For example, it may affect an individual’s ability to feel safe and/or develop trusting relationships with professionals. A DHR that uses a trauma-informed approach will see beyond a victim and perpetrator’s presenting behaviours and ask, ‘What did this person need?’ rather than promoting victim-blaming narratives of ‘What was wrong with this person?’ and ‘Why did they not leave?’.
Professionals engaging with the DHR will also be exposed to information that could be traumatising and trigger a trauma response. The DHR Chair must work to create a psychologically safe environment for professionals engaging in the DHR To ensure DHR’s are conducted in a psychologically safe environment, DHR Chairs should consciously use sensitive language when discussing the death, provide trigger warnings prior to the description of graphic content and actively ensure the well-being of the panel members is not negatively affected by their involvement in the DHR.
All local DHR Chairs, Panels and CSPs, should ensure that they use trauma-informed language and agree a ‘shared language’ when creating the Terms of Reference. This is particularly important in instances when a review is related to a victim who died by suicide, as it helps to create a safe and compassionate environment and aims to prevent re-traumatisation.[footnote 12]
8b. Victim-Centred Approach
DHRs must use a victim-centred approach. If a DHR is not victim-centred it can easily become a de-humanising exercise, and in the worst cases, continue to perpetuate the power dynamics of domestic abuse that existed in the victim’s life. To ensure the DHR employs a victim-centred approach, throughout the process, DHR Chairs must:
- ensure that family, friends and the community of the victim are treated as crucial to the DHR process;
- not accept perpetrator narratives without challenge;
- involve experts to better understand the victim’s experience; and
- guard against victim blaming narratives.
Setting the tone of a victim-centred approach at the beginning of the DHR by using a ‘pen portrait’[footnote 13] is good practice as it gives the reader a sense of what the victim was like, their likes and dislikes, their hobbies and how their family and friends described them. If the victim’s families and friends have decided not to write their own pen portrait, the DHR Chair can outline what they have learnt about who the victim was.
The DHR should challenge any agency narratives stating ‘the victim did not engage with services’. Instead, the DHR Chair should explore if there were barriers that the victim faced when accessing services or if there are other service provision models that could have been used to support or safeguard the victim.
8c. Involvement of family, friends, and communities
The quality and accuracy of a DHR is likely to be significantly enhanced by the involvement of family, friends and communities.[footnote 14] Families should be given the opportunity to engage closely with the DHR and should be treated as a key stakeholder. The benefits of involving family, friends and the communities of the victim and where appropriate, the perpetrator’s, include obtaining information about the nature and extent of the abuse which may not have been shared with agencies. It can also humanise and help to better understand the victim.
The DHR Panel should be aware of the risk of ascribing a ‘hierarchy of testimony’ regarding the weight they give to statutory agencies, the voluntary sector and family and friends contributions.
Family and friends may not want to engage with the DHR, in these cases, the DHR Chair should reach back out to the family/friends before the DHR is finalised and sent to the Home Office to see if their position has changed and offer another opportunity to engage.
In some cases, family and/or friends may attempt to continue to present the narrative of the perpetrator. Where the domestic abuse has been situated in a wider family context, some family members or friends may fear engaging in the DHR for risk of reprisals from those who perpetuate harmful narratives and behaviours. For example, in cases where ‘honour’-based abuse has taken place. The DHR Chair and CSP should be highly sensitive to these issues, apply professional curiosity and ensure those who would like to engage in the DHR are given the opportunity to, with risk assessments and safety planning in place where necessary.
The safety of individuals involved in a DHR must take precedence. Therefore, adult and/or child safeguarding risk assessments, in line with local practices, must be conducted to ensure the safety of said individuals. The identified perpetrator(s) of the death may not be a convicted criminal or have any criminal charges brought against them relating to the death, meaning the perpetrator and associated family and friends may still be present and pose a risk to the victim’s family and friends, notably the victim’s children.
The nine requirements outlined in Figure 2 need to be specifically outlined in the DHR and if they have not been met, an explanation for why must also be included and communicated to the family and friends. Annex G in the DHR toolkit presents the requirements in a checklist form.
Figure 2: Nine requirements for engaging family and friends in the DHR
| Requirement | Responsibility |
|---|---|
| 1. Family/friends must be notified when a Scoping Review is commissioned. If the CSP is recommending that a DHR must not be conducted, the views of the family and friends on this decision must be included in the Scoping Review. | CSP |
| 2. When a DHR is commissioned the CSP must ensure that family and friends of the victim are given the Home Office leaflet and referred to a specialist and independent advocacy service. Children must also be given specialist help and an opportunity to contribute as they may have important information to offer. | CSP |
| 3. Once a DHR Chair has been appointed, they must write to the family and friends to introduce themselves, offering the opportunity to engage with the DHR. The DHR Chair must explain clearly how the information disclosed will be used, anonymised and whether this information will be published. | DHR Chair |
| 4. Adjustments must be put in place throughout to ensure that family/friends are given the opportunity to engage with the DHR. This might entail the use of interpreters, translated versions of documents, agreeing a reasonable timeframe for the family to review the terms of reference and final DHR. | CSP and DHR Chair |
| 5. Family/friends must be given the opportunity and adequate time to review a draft of the terms of reference for the DHR and to share any feedback with the DHR Chair and panel. | DHR Chair |
| 6. Family/friends must be given the opportunity to attend and share information at DHR panel meetings or with the DHR Chair alone. | DHR Chair |
| 7. The DHR Chair must agree with family/friends how regularly they would like to be updated on the progress of the DHR. | DHR Chair |
| 8. Family/friends must be given a copy of the draft DHR before submission to the Home Office and the opportunity to provide feedback on the DHR. If there are disagreements between family/friends and the DHR Chair and local panel this must be recorded in the DHR. | DHR Chair |
| 9. The DHR Chair must hand over contact details of all family and friends to the CSP, who must update family/friends on the implementation of the DHR Action Plan. | CSP |
8d. Engagement with perpetrators
A note on language: in reviews where the death was a homicide, the perpetrator is the perpetrator of the homicide. In reviews where the death was a suicide, or as a result of neglect, or where circumstances surrounding the death are unclear, the perpetrator will be referred to as to the perpetrator of domestic abuse. This should be made clear in the DHR.
A DHR is a learning exercise, and this is the approach that should be taken when engaging with perpetrators. Before including information about the perpetrator in the DHR, the DHR Chair and DHR Panel should consider what they can learn from this information to ensure that the DHR does not repeat the perpetrator’s narrative unchecked.
The DHR should consider what interventions could have been in place for the perpetrator to prevent them causing harm. Putting all the focus for interventions on the victim, and none on the perpetrator can create a victim blaming narrative, highlighting a lack of understanding and expertise in the dynamics of domestic abuse and the challenges facing victims of domestic abuse, which is essential when conducting a DHR.
Before approaching a perpetrator, the DHR Chair should discuss their plans with the family and friends of the victim and take their views into consideration. Any concerns for the safety of family, friends or reviewers may mean it is not possible to engage the perpetrator in the DHR. This may be particularly relevant when conducting a review for a death that has not been ruled as a domestic homicide.
Whilst it can be beneficial to engage perpetrators to understand their perspective, DHR Chairs should be careful not to focus unduly on their views. A DHR is about identifying and implementing learning from these events. Therefore, if engagement with the perpetrator is taken forward, the DHR should focus on what interventions they did or did not receive and their views on them. The purpose of this focus is to create a learning opportunity for agencies, but to set boundaries in the interview.
8e. Cases not ruled as homicide
A significant proportion of DHRs will be cases where a victim of domestic abuse has died by suicide. Reviewing suicides linked to domestic abuse is an important step in building the evidence base and understanding of the risk factors for victims and perpetrators of domestic abuse where a victim takes their own life.
To identify suicide cases which should be considered for a DHR CSPs need to establish strong links with Public Health partners and local real-time suicide surveillance processes.
When commissioning a review on a domestic abuse-related death that does not have any ongoing criminal justice proceedings, the CSP and DHR Chair must work closely with police to understand whether there are any intentions to open investigations pertaining to possible criminality in the future. The CSP and DHR Chair can then ensure they are making informed decisions about disclosures and engagement with the perpetrator(s) of domestic abuse identified in the review and avoid impacting any future investigations.
The DHR Chair, CSP and local panel should also be mindful that for reviews where there are no criminal justice proceedings the family of the victim will not have been assigned a Family Liaison Officer, therefore ensuring specialist and independent advocacy referrals are made at the earliest opportunity is crucial, and the CSP may need to consider if there are any other referral pathways in place locally to support the family as they navigate the complex challenges and bereavement in complex circumstances.
All local areas have a suicide prevention strategy overseen by the Director of Public Health, and the DHR Chair and local panel must ensure that those with responsibilities for the local suicide prevention strategy are aware of the DHR and given the opportunity to provide their local knowledge and expertise.
8f. Analysis
The Analysis section within the DHR should examine how and why events occurred, information that was shared or not shared, the decisions that were made, and the actions that were taken (or not taken). It can consider whether different decisions or actions may have led to a different course of events. The analysis section should address the terms of reference and the key lines of enquiry within them. It is also where any examples of good practice should be highlighted. We encourage DHR Chairs to consider any relevant research to support the analysis.
The DHR Chair and the DHR Review Panel should consider equality and diversity issues throughout the DHR. All DHR Chairs and Panels must comply with the requirements set out in the Public Sector Equality Duty. The Equality and Diversity section in the DHR must not merely cite data but analyse how each protected characteristic impacted the individual and the events that led to the death. DHR Chairs must explicitly cite the sources that they have used. As outlined in Section 4 of the Equality Act 2010, legally recognised protected characteristics include: age; disability; gender reassignment; marriage and civil partnership; pregnancy and maternity; race; religion and belief; ethnicity; sex and sexual orientation.
These protected characteristics may impact how an individual’s experiences and interacts with services and agencies. Therefore, the DHR should reflect these in the information it documents about the victim’s life. It is not expected that these characteristics will only be relevant for minority groups, instead they should be explored for all individuals. More than one protected characteristic may impact an individual’s personal experience. Therefore, the DHR Chair and Panel members should ensure equality and diversity are considered as part of this.
Other vulnerabilities that are not captured by protected characteristics should also be considered, such as individuals who are known to have been victim to different form of abuse throughout their lives. In this section you may also want to consider insecure immigration status and geographical factors, for example, a domestic abuse victim living in a rural community may not have the same access to services as a victim living in a city.
Panel members and agencies involved in the DHR should take tangible actions to mitigate against any bias that may impact the conduct and outcome of the review, consciously or unconsciously. There should be reference to this within the DHR.
9. Parallel Reviews
In instances where a death could fall in scope of multiple statutory or non-statutory reviews, the CSP and the DHR Chair should inform the relevant boards that a DHR is being considered at the earliest opportunity.
Early conversations at the outset will limit duplication, for both the professionals involved in the reviews and the family and friends of the victim, if they are required to participate. It can also help to identify the most appropriate way to foster professional and agency learning that can be shared by both reviews. Where appropriate, a joint review can be undertaken however, it is important for safeguarding partners to organise how reviews can be successfully combined while still meeting the core purpose of each.
The Terms of Reference of the DHR should reflect any decision to conduct joint or parallel reviews. The Terms of Reference should be shared with the agencies involved, and a consensus reached to ensure the key requirements of both processes are clearly identified and met. Joint working ensures that all aspects of the review can be addressed and that the identified processes complement and strengthen each other.
It may be necessary for the DHR Chair or the Scoping Review Panel to consider pausing the DHR to allow other investigations to take place.
In the event it is deemed appropriate for a parallel review to take place, the guidance in 8a-8d should inform ways of working.
9a. Mental Health Homicide Reviews (MHHR)
Where an DHR is being considered and it is confirmed/or possible that the perpetrator was in receipt of secondary mental health services, both a DHR and MHHR can take place in parallel.
NHS England is responsible for carrying out an MHHR. These deaths are investigated using the NHS England Patient Safety Incident Response Framework and supporting guidance.
The DHR Chair should make early contact with the relevant NHS England lead. Relevant contact details can be found in the Glossary of Key Contacts.
9b. Safeguarding Adult Reviews
A Safeguarding Adults Board (SAB) is required to arrange a Safeguarding Adult Review (SAR) of a case involving an adult in its area with needs for care and support (whether or not the local authority has been meeting those needs) if there is reasonable cause for concern about how partner agencies worked together to safeguard the adult. SAB’s are also required to carry out a SAR in circumstances where the adult has either (1) died and the SAB knows or suspects the death resulted from abuse or neglect (whether or not they knew about or suspected the abuse or neglect before the adult died) or (2) is still alive and the SAB knows or suspects the adult has experienced serious abuse or neglect. More information on how SAR links with other reviews can be found in the Care and support statutory guidance.
9c. Child Safeguarding Practice Reviews
The purpose of Child Safeguarding Practice Reviews (CSPR), at both local and national level, is to identify improvements to be made to safeguard and promote the welfare of children. Learning is relevant locally, but it has a wider importance for all practitioners working with children and families and for the government and policy officials. Understanding whether there are systemic issues, and whether and how policy and practice need to change, is critical to the system being dynamic and self-improving.
Alongside any national or local reviews, there could be a criminal investigation, a coroner’s investigation and/or professional body disciplinary procedures. The Panel and the safeguarding partners should have clear processes for how they will work with other investigations, including DHRs and work collaboratively with those responsible. This is to reduce burdens on and anxiety for the children and families concerned and to minimise duplication of effort and uncertainty.
If the victim was aged 16-18, it is possible a DHR may be conducted alongside a Child Safeguarding Practice Review. This may also be appropriate where separate review processes arise from a single or linked incident.
Section 16C(1) of the Children Act 2004 (as amended by the Children and Social Work Act 2017) states: Where a local authority in England knows or suspects that a child has been abused or neglected, the local authority must notify the Child Safeguarding Practice Review Panel if – (a) the child dies or is seriously harmed in the local authority’s area, or (b) while normally resident in the local authority’s area, the child dies or is seriously harmed outside England.
9d. Serious Further Offence Reviews
In the event an individual has been charged with a Serious Further Offence (SFO)[footnote 15], the Probation Services (PS) will carry out an internal review to determine whether the practice standards were met, if deficiencies were identified and if necessary how these will be addressed. This will inform the completion of a timely and comprehensive IMR which directly addresses the specific Terms of Reference of the DHR. The lead Senior Manager for the PS should liaise with the DHR Chair to and facilitate adequate information sharing including in relation to liaison with victims.
10. Criminal investigations
It is necessary for the DHR Chair to determine if there are any criminal proceedings associated with the death at the earliest opportunity.
It is good practice to ensure scoping related to ongoing criminal proceedings is carried out during the Scoping Review stage. To do this the DHR Chair should contact the Crown Prosecution Service (CPS) Single Point of Contact (SPOC). Regional SPOC details can be found in the Glossary of Key Contacts.
Early contact with the CPS, and other appropriate justice agencies (e.g. HM Coroner, the police, Independent Police Complaints Commission (IOPC)), will ensure the DHR and the separate criminal proceedings can be sequenced in the most suitable way.
The CSP should consider inviting the police officer on the case to brief the Scoping Review Panel or the DHR Panel if it has been established.
10a. Decision to pause the DHR
If, following representations from the police, it is agreed by the DHR Panel to delay progressing the DHR, it must be concluded without delay as soon as the criminal proceedings have finished so lessons can be identified and rapid action taken to address them. The family of the victim should be informed of the decision to delay the DHR at the earliest opportunity.
Before a criminal trial has taken place, the DHR Chair can carry out preliminary work to prepare for the DHR. This may include commissioning and analysing IMRs and drafting a first iteration of a chronology. The DHR Chair must avoid speaking to potential witnesses whilst doing so.
When considering interviews as part of the preliminary work, the DHR Panel must consider that family members, friends and other support networks may be potential witnesses, or even defendants in a future criminal trial. The DHR Chair will need to discuss the timescales for interviews with the police and take guidance regarding any ongoing criminal proceedings.
Any appeals lodged following the conclusion of criminal proceedings should not delay the submission of a DHR to the Home Office for quality assurance.
10b. Conducting a DHR alongside criminal proceedings
If a DHR is anticipated to run in parallel to a criminal investigation or prosecution, the DHR Chair should inform the police. This will allow the police the opportunity to express their views and input into the DHR Terms of Reference before they are finalised.
10c. Disclosure
Conducting a DHR in parallel to criminal proceedings is likely to incur disclosure implications[footnote 16], which need to be carefully managed. The DHR Chair is responsible for establishing and maintaining regular contact with the police, who may defer to the relevant disclosure officer. This will aid the development of a robust process for disclosure of any relevant materials.
If there are any disclosure issues, they must be discussed with the police, the CPS and the HM Coroner’s representative as appropriate; and provisions outlined in the Criminal Procedure and Investigations Act 1996 must be followed.
Dependent on the case, material gathered during a DHR may be capable of assisting the defence case and is material to which the defence may seek to gain access. It is important to consider that interviews with other agency staff, documents, case conferences and other related documents may all be disclosable.
Where suicide has occurred following domestic abuse, the DHR may encounter material which suggests there is a connection between the domestic abuse and the suicide. In most cases, for the purposes of charges of manslaughter or murder, it cannot be said that suicide was caused by another person. However, in some cases the actions of the perpetrator may have caused a recognised psychiatric injury to the victim, or the abuse may have been so extreme as to mean the victim’s actions were not voluntary. In those cases, manslaughter or murder may warrant investigation. The DHR may wish to consider whether such an investigation has taken place or not, and whether the material the review has seen has also been considered for these purposes by the police.[footnote 17]
11. Coronial Inquests
When conducting a DHR, the coroner’s investigation must also be considered where relevant. The relevant coroner’s office should be informed by the DHR Chair or CSP that a DHR has commenced in relation to a death. Where the perpetrator is alive and criminal proceedings (for a homicide offence or a related offence) are being undertaken, the coroner’s inquest will be suspended whilst awaiting the outcome of the trial. In these cases, the coroner will likely want to have access to the final published DHR and may also wish to access relevant underlying information.
The coroner will require sufficient disclosure of information and evidence for them to carry out their statutory duties. The public interest in the pursuit of an appropriately detailed inquest may outweigh a public interest claim for non-disclosure of a DHR into a death, especially when the disclosure is to a coroner instead of the public. Therefore, coroners should expect a greater level of disclosure made to them, so that they may properly assess the scope of an inquest and the witnesses to be called, including IMRs and the draft DHR. When sharing an unpublished DHR, the DHR Chair must ensure the coroner is aware that the DHR, and its findings, may change significantly after receiving feedback from the Home Office Quality Assurance Board.
Early notification of the DHR to the coroner will help manage the exchange of information and the identification of any data sharing or disclosure concerns.
Before publication of the final DHR or sharing any drafts with family members, discussions should be held in advance to ensure no sensitive information is disclosed inappropriately, or in a way which could cause distress. For example, the post-mortem report on the victim may form part of the information provided by the police to the DHR. This should not be shared with a wider audience without the permission of the coroner.
12. Conducting a DHR in Wales: The Single Unified Safeguarding Review (SUSR)
The Single Unified Safeguarding Review (SUSR) is a single review process incorporating all homicide reviews in Wales. The SUSR statutory guidance has been cross referenced with the DHR guidance to ensure it will deliver everything required from both the Home Office and Welsh Government perspectives. The SUSR is delivered through the Safeguarding Boards and in domestic abuse-related deaths, with the Community Safety Partnership for the area.
While DHRs are to be delivered in Wales, through the Single Unified Safeguarding Review process, there are certain additional steps that need to be undertaken to ensure the DHR legislative requirements are met for reviews in Wales. These are stipulated in the Single Unified Safeguarding Review process and include the submission of the final review to the Home Office Quality Assurance Panel and to the Office of the Domestic Abuse Commissioner.
The Single Unified Safeguarding Review Statutory Guidance can be read in full at Hyper link will be provided.
Background
The Single Unified Safeguarding Review happens in a unique delivery and legislative context. It is essential for devolved and non-devolved organisations to work in partnership in Wales, at all levels, to deliver the best possible outcomes for people. This ensures that relevant lessons are learnt across the governance structures and required changes and adjustments are made where appropriate locally, regionally, and nationally.
This approach also embodies a broader agreement that partners should work together across disciplines and partnership arrangements in Wales to share learning and prevent harm. Organisations in Wales should work together across Community Safety Partnerships, Regional Safeguarding Boards, Public Service Boards etc to ensure learning from reviews (both individual reviews and thematic learning) is shared and acted on appropriately to protect people and communities from harm.
The Government of Wales Act 1998 (GoWA 1998) provided for the transfer of executive functions from UK Government Ministers to the National Assembly for Wales (now Senedd Cymru). Under GoWA 2006, those functions were transferred from the National Assembly for Wales to the Welsh Ministers. The Welsh Ministers now exercise the majority of the executive and subordinate legislative powers in relation to local government whether those powers are conferred by an Act of Senedd Cymru or an Act of the UK Parliament.
Section 108A of and Schedules 7A and 7B of GoWA 2006 establish the basis of the legislative competence of the Senedd to make primary legislation. Schedule 7A specifies the areas of policy in respect of which only Parliament can legislate. Any area not listed within Schedule 7A is within the legislative competence of the Senedd; Schedule 7B contains general restrictions on the way in which the Senedd may exercise its legislative competence.
Accordingly, education and training, health services, housing, local government, social welfare, and Fire and Rescue, are therefore within the legislative competence of the Senedd. It can therefore be seen, in order for any review to be undertaken in Wales, it needs to ensure it is compatible with the devolution settlement and relevant processes established in Wales. As an example, on average, over 80% of recommendations made within Domestic Homicide Reviews conducted in Wales involve devolved Welsh authorities and yet Welsh Ministers were historically not engaged in DHRs. It is therefore essential for Welsh Ministers to be aware of recommendations arising from reviews, which are within their portfolio areas, to ensure learning identified is embedded and policies and processes changed where necessary.
13. Anonymisation
DHRs must be anonymised. Requirements include:
-
Pseudonyms for all individuals referenced in the DHR. In some cases, the family of the victim may request that victim’s real first name is used, if this request is accepted all other anonymisation requirements should remain;
-
Exact dates should not be used, only the month and year are required;
-
Place names, names of buildings, schools etc should not be used;
-
For children, sex or specific age should not be referred to.
-
To maintain anonymity and prevent unnecessary risks to panel members, members of the DHR Panel should not be named in the DHR. However, the names of the respective agencies should be included.
14. Data protection
Following the obtained consent from all parties involved with regards to information sharing, the DHRs should remain confidential and have a restricted audience until they have been approved by the QA Board. All documentation should be marked as ‘Official-Sensitive’ until publication.
The production and publication of DHRs are subject to the Data Protection Act 2018. The DHR Chair and relevant partners will need to consider whether any sections of the DHR need to be redacted in order to comply with data protection legislation. They must ensure that all information intended for publication does not undermine ongoing criminal investigations, proceedings or jeopardise the safety of any person, such as the family of the victim or vulnerable witnesses. .
For the purpose of a DHR, the lawful basis for processing data are as follows (this applies to all DHRs, including where the victim died by suicide, neglect or in unexplained circumstances):
General processing (as defined by the General Data Protection Regulation):
-
General Data Protection Regulations (GDPR) Article 6
-
Art 6(1)(c) Necessary for compliance with a legal obligation.
-
Art 6(1)(e) Task carried out in the public interest or in the exercise of official authority
-
Art 6(1)(f) Legitimate Interest
-
If processing involves special categories of data, GDPR Article 9
-
Art 9(2)(c) Vital interests of the data subject or a third party where they are incapable of giving consent.
-
Art 9(2)(g) Necessary for reasons of substantial public interest.
-
GDPR Art 9(2)(g) requires a basis in UK law, which is provided by Section 10(3) of the Data Protection Act 2018 (DPA 2018).
This in turn refers to the need to meet a relevant condition in Part 2 of Schedule 1 of the DPA 2018. The relevant condition is:
-
Condition 10 – preventing or detecting unlawful acts
-
Condition 18 – safeguarding of children and of individuals at risk
Processing for law enforcement purposes (processing by competent authorities as defined by the Data Protection Act 2018):
- DPA 2018 – use of personal data, Part 1 Section 31
For the purposes of this Part, “the law enforcement purposes” are the purposes of the prevention, investigation, detection or prosecution of criminal offences or the execution of criminal penalties, including the safeguarding against and the prevention of threats to public security.
-
DPA 2018 – Schedule 1, Part 2(6) for the processing of special category data (Statutory etc and government purposes)
-
6(1) This condition is met if the processing—
-
(a) is necessary for a purpose listed in sub-paragraph (2), and
-
(b) is necessary for reasons of substantial public interest.
-
-
(2) Those purposes are—
-
(a) the exercise of a function conferred on a person by an enactment or rule of law;
-
(b) the exercise of a function of the Crown, a Minister of the Crown or a government department.
-
In accordance with section 35(2) DPA 2018,
- 35(2)(b) The processing is necessary for the performance of a task carried out for that purpose by a competent authority.
In the case of sensitive processing,
-
35(5) The processing is strictly necessary for the law enforcement purpose, and meets a relevant condition in Schedule 8. The relevant condition is:
-
Condition 1 – statutory etc purposes
-
Condition 4 – safeguarding of children and individuals at risk
-
The Department of Health and Social Care encourages clinicians and health professionals to cooperate with DHRs and disclose all relevant information about the victim and, where appropriate, the domestic abuse perpetrator. Where record holders consider full disclosure of information not appropriate (e.g. due to confidentiality obligations or other human rights considerations), the following steps should be taken:
- Record holders should inform the DHR Panel about the existence of relevant information to an inquiry in all cases; and
- Discuss their concerns about disclosure with the DHR Panel. Attempts to reach agreement on the confidential handling of records or partial redaction of record content should be made.
The Department of Health and Social Care is clear that, where there is evidence to suggest that a person is responsible for the death of the victim, the greater public interest should be prioritised over their right to confidentiality.
15. Home Office Quality Assurance Board
The Home Office Quality Assurance Board (‘the QA Board’) should review all DHRs prior to publication. The purpose of the QA Board is to consider whether the DHR has met the requirements set out in the DHR statutory guidance and to consider any gaps in the DHR. Where gaps are identified, the QA Board will provide feedback to the CSP. DHRs cannot be published without approval from the QA Board.
Criteria used by the QA Board to determine if a DHR is ready for publication:
- The scope and Terms of Reference are appropriate;
- The DHR employs a trauma-informed approach;
- DHR is victim-centred;
- The views of the family, friends and the community are reflected and if this is not possible, an explanation of why they did not engage is provided;
- There is comprehensive analysis of the information gathered;
- Appropriate learnings are identified; and
- Compliance with the template and guidance.
Where the criteria have not been met, the QA Board may request a DHR is resubmitted for review before it can be published. Where the criteria are met but the QA Board identify areas for improvement, CSPs are expected to reflect the changes requested before publication.
The QA Board is chaired by the Home Office and includes membership from statutory agencies and domestic abuse experts. The QA Board meets every month to discuss DHRs and any Scoping Reviews that have been submitted to the Home Office over the previous month where the CSP is recommending that a DHR should not be commissioned.
15a. Decisions not to conduct a DHR
Where a CSP is proposing not to conduct a DHR, the QA Board will consider whether the case meets the criteria for a DHR as per the Domestic Violence, Crime and Victims Act 2004 and review the rationale provided in the Scoping Review. The QA Board will provide feedback where they believe a DHR should be commissioned.
The recommendation to conduct a DHR, along with the rationale, will be shared with the CSP by the QA Board Secretariat. If the CSP continue to maintain that a DHR should not be commissioned, the decision will be escalated to the Home Secretary who may choose to direct the CSP to conduct a DHR.
Terms of Reference for the QA Board are included in Annex H.
16. Publication
Once the final copy of the DHR has been shared with the family and friends, it must then be sent to the Home Office and Domestic Abuse Commissioner, and will be published on the Domestic Homicide Review Library.
Publication requirements for the DHR Library are:
- The DHR should be converted to a PDF document and be smaller than 20 MB in size and include the following annexes;
- The final QA Board feedback letter should be attached to the end of the DHR as an annex; and
- The DHR Action Plan should be added to the DHR as an annex. This should include all implementation updates and note that the action plan is a live document and subject to change as outcomes are delivered. The Action Plan template and guidance can be found in Annex B.
Community Safety Partnerships should continue to publish the DHR on their own websites or clearly signpost and provide a link to the DHR Library. If CSP’s choose to publish on their own website, it must be the same version as that published on the DHR Library.
16a. Decision to not publish a DHR
There will be a small number of DHRs that are not published in their entirety or at all. The recommendation not to publish should be based on a risk assessment for the safety of family members and friends of the victim, in addition to the DHR Panel members. All requests to not publish a DHR (in part or full) should be submitted to the QA Board alongside the draft DHR. This submission should set out what the CSP will publish (e.g. a redacted version of the DHR and action plan) and how the CSP will share learning locally with professionals and the community. The QA Board will review the request and share feedback on the publication decision and plans with the CSP. Family and friends should also be consulted on the decision not to publish the DHR.
16b. Amending a published DHR
It is possible that further information may emerge after a DHR has been published that is pertinent to the findings of the DHR. In these scenarios it is the responsibility of the CSP to decide whether the DHR needs to be updated. If the CSP decide to update the DHR, they must notify the Home Office to remove the DHR from the DHR Library. Any amendments and additions to the DHR must be clearly signposted in the document. The updated DHR will need to be resubmitted to the QA Board before it is published. In some circumstances, the change may be minimal, therefore the Home Office may agree that a DHR can be updated without going back to the QA Board, provided amendments are clear and it is noted that it has not been seen by the QA Board.
Section 3: Implementation of Learning – Making the Future Safer
17. National and local oversight and implementation of learning
Action plans and recommendations are a vital part of the DHR process, and it is crucial that sufficient focus and attention is given to their development and implementation to ensure learning is meaningful, relevant and achieves change to prevent further abuse and homicide. That is why formal roles for Police and Crime Commissioners (PCCs) and the Domestic Abuse Commissioner (DAC) in the oversight of the implementation of learning in DHRs have been introduced.
DHRs are rooted in the community of the victim and perpetrator and each DHR must have an accompanying action plan which addresses the local learning identified in the DHR with targeted and measurable actions that have clear outcomes that will make a difference. DHRs can also make national recommendations where policy change is needed on a national scale. These national recommendations will be collated, analysed and presented to the Home Office by the Domestic Abuse Commissioner. The implementation of accepted national recommendations will be subject to Ministerial governance as part of oversight of VAWG within the Home Office.
18. Role and responsibility of the DHR Chair
The DHR Chair is responsible for managing the DHR process and ensuring all avenues that may provide learnings to prevent future domestic abuse-related deaths are explored. For example, in collaboration with the DHR Panel, the DHR Chair must work to identify the learning from analysis of the death. The DHR Chair must consider what actions will lead to measurable outcomes which will improve safeguarding for victims and risk management of perpetrators.
The DHR Chair should co-produce the final DHR with the DHR Panel. For further detail on conducting and producing a DHR, please refer to Section 2:6 ‘Conducting a Domestic Homicide Review’ and Section 2:7 ‘Compiling a Domestic Homicide Review’.
The DHR Chair is responsible for cultivating and maintaining relationships amongst the DHR Panel and between the DHR Panel and participating agencies, organisations and individuals. Therefore, any conflict of interest should be declared at the point of recruitment and when it arises during the DHR process. The DHR Chair is also responsible for leading on engagement with the family and friends of the victim.
The Chair should provide support where necessary to the CSP as they develop the action plan. The DHR Action Plan must reflect any gaps identified during the DHR and should seek to put in place measures to reduce the risk of another tragedy occurring in similar circumstances.
19. Role and responsibility of the Community Safety Partnership
The Chair of the CSP holds responsibility for establishing whether a homicide is to be the subject of a DHR, set out in section 1(2) of the 2004 Ac. This decision should be taken in consultation with local partners who work with victims of domestic abuse and understand the dynamics of domestic abuse as defined in the 2021 Act. This assessment will assist in identifying appropriate DHR Panel members. When considering whether to conduct a DHR, CSPs should contact relevant bodies to establish the existence of any other ongoing reviews, such as a child Serious Case Review (SCR) (Child Practice Review in Wales), Safeguarding Adults Review (SAR) or Mental Health Investigation (MHI).
The CSP has overall responsibility for the DHR and the creation and implementation of the action plan. As the action plan is being developed, the CSP should work collaboratively with the DHR Chair and local DHR Panel to engage and work with local agencies for who actions have been identified. The CSP should ensure that the actions developed are appropriate, with an identified owner who will be responsible within the organisation. To ensure that the action is implemented in a timely manner and is working to achieve the intended outcomes, the CSP should develop a governance structure when working with partners, so as to ensure effective delivery.
The CSP must engage with the local Police and Crime Commissioner (PCC) to consider levers and governance for the delivery of the draft action plan. The PCC may assist in identifying where wider application of the action plan would be beneficial; convene agencies to identify how the plan and recommendations should be disseminated more widely; and identify resources to assist with the delivery of the action plan were appropriate. Pre-existing local governance structures may be utilised to develop insight into how DHR actions and recommendations are being delivered to achieve change. Structures in place to prevent and reduce crime will vary locally. Examples may include multi-agency partnerships such as Domestic Abuse Local Partnership Boards, Integrated Care Boards, Health and Wellbeing boards, or be a collaboration of several different partnership forums.
The CSP should seek to disseminate learnings from the DHR to local professionals e.g., through a learning event. Early learning can be shared whilst the DHR is still underway to aid continuous improvement to delivery of services. A learning event should be held after the DHR has been published to share the final action plan with local professionals, agencies and Domestic Abuse Partnership Boards. This will maintain momentum across agencies to ensure that meaningful change is embedded following the death. It is good practice to include the Police and Crime Commissioner (PCC) and Domestic Abuse Commissioner (DAC) in post publication learning events to increase the opportunity for cross border learning.
20. Role and responsibility of the Police and Crime Commissioner
Police and Crime Commissioners were introduced in 2012 to make the police more accountable in their areas through oversight by a directly elected individual. Whilst police forces are operationally independent, PCCs are responsible for policing within their area and aim to cut crime and deliver an effective and efficient police service within their force area. PCCs ensure community needs are met as effectively as possible and improving local relationships through building confidence and restoring trust. They work in partnership across a range of agencies at local and national level to ensure there is a unified approach to preventing and reducing crime.
As part of their wider role, PCC’s responsibilities align to the desired outcomes of DHRs, therefore their involvement in supporting the process is key to improving local responses to prevent domestic abuse and homicide. These responsibilities include:
- commissioning services to support victims of crime;
- working with other organisations, including criminal justice partners to deliver a joined-up approach to local priorities;
- and improving community safety.
PCCs should maintain a strategic oversight of the DHRs across their areas and support knowledge sharing. Due to the variations in structure, size and function of PCCs, the mechanisms and structures which the PCC adopts for this oversight of DHRs will vary. The CSP must ensure that they actively engage their local PCC, involving them in the drafting process of action plans and provide a quarterly progress update.
The PCCs should act as a facilitator to convene partners and provide strategic advice should the CSP require assistance in order to develop or deliver upon the action plan.
Following the publication of the action plan, the PCC should engage the CSPs on knowledge sharing events and publications to disseminate the learning across relevant partners. The PCC should consider drawing together findings from multiple DHRs to support knowledge sharing.
21. Role and responsibility of the Domestic Abuse Commissioner
The role of the Domestic Abuse Commissioner (DAC), as set out in the Domestic Abuse Act 2021, is to drive improvements in the response to domestic abuse, and to hold local and national Government to account. The DAC is independent of Government and specified public authorities (including Government Departments) have a duty to cooperate with the DAC and to respond to their recommendations. The 2021 Act sets out that the Domestic Abuse Commissioner’s statutory function is to encourage good practice in:
- The prevention of domestic abuse
- The prevention detection, investigation and prosecution of offences involving domestic abuse
- The identification of people who carry out domestic abuse, are victims of domestic abuse and children affected by domestic abuse
- The provision of protection and support to people affected by domestic abuse
The DAC will play an active role in the DHR process at both a national and local level. The DAC has responsibility for identifying key themes and learning opportunities from DHRs, advising the Government on where to make improvements at a national level, and supporting local agencies and national bodies to implement recommendations.
At a local level, the DAC will ensure the dissemination of learnings and insight through routine engagement with PCCs and CSPs, supporting partnership development and cross border learning networks. The DAC will engage with CSPs to understand the progress of delivery of action plans and be a point of escalation for instances where there are obstacles to implementation of actions or recommendations. This regional learning will supplement information on national learnings and allow a fuller picture on the challenges to implementing action plans.
At a national level, the DAC will compile an annual report that considers key themes from DHRs published that year and identify areas where the Government must consider policy changes. The report will also consider how effective the implementation and impact of DHR learning has been. The DAC will put forward their findings to Government Departments and national statutory agencies where changes need to be made at national level to bolster safeguarding of victims and risk management of perpetrators.
22. Role and responsibility of the Home Office
The Home Secretary has overall responsibility for DHRs and is able to direct a specified person or body set out in section 9(4) of the Domestic Violence, Crime and Victims Act 2004 to establish, or to participate in, a DHR (see section 9(2)). The Home Office is responsible for convening Government Departments to facilitate a whole-systems approach to implement and monitor national recommendations. This will be carried out through inter-ministerial governance structures, overseen by Home Office Ministers.

Figure 3: National and local oversight structures for DHR recommendations and actions.
DHR Toolkit
Annex A: DHR Template
TITLE PAGE OF DHR
- Name of the Community Safety Partnership
- Victim’s pseudonym and month and year of death
- Author’s name
- Date of publication
1. LIST OF CONTENTS PAGE
2. PEN PORTRAIT OF VICTIM
Family and friends to be given the opportunity to write a pen portrait of the victim.
A Pen Portrait is ‘a description of someone as a person (e.g. their personality, their likes and dislikes), their history (e.g. over their life course or more recently) as well as their needs or experiences’.
3. DHR CHAIR + CSP CONDOLONCES
4. CONFIDENTIALITY AND ANONYMITY STATEMENT
Include pseudonym/s agreed with the family and used in the DHR to protect the identity of the individual(s) involved. Names rather than letters are encouraged as it is more humanising.
5. EXECUTIVE SUMMARY
A high level summary of the death, analysis, and lessons learnt. This should be approximately 2-4 pages.
6. TERMS OF REFERENCE
A non-exhaustive list of factors that the DHR Chair should consider when developing the scope of the DHR includes the time period under review; agencies that had been involved; a determination of MARAC involvement; terms of engagement with family and friends; public and media attention and engagement; equality and diversity; other reviews into the death; and whether there have been other DHRs in the same local authority area and any relevant learning they offer.
7. BACKGROUND INFORMATION (THE FACTS)
- A synopsis of the homicide (what actually happened and how the victim was killed).
- Details of the Post Mortem and inquest and/or Coroner’s inquiry if already held. State the cause of death.
- Members of the family and the household. Who else lived at the address and, if children were living there, what their ages were at the time (to ensure anonymity, the children’s sex should not be given).
- How long the victim had been living with the perpetrator(s). If a partner/ex-partner, how long they had been together as a couple.
- Details of any criminal charges including the date and outcome of the trial, and sentence given.
- If the review is being undertaken into a victim that died by suicide, state on what basis this was considered to meet the criteria to undertake the review.
8. AGENCY OVERVIEW
An overview that summarises what information was known to the agencies and professionals involved about the victim, the perpetrator and their families. Including whether there was no contact with the victim and perpetrator and any other relevant facts or information about the victim and perpetrator, for example psychological assessments.
9. COMBINED CHRONOLOGY
There must be a combined agency chronology (rather than outlining each agency’s contact in turn).
If the family structure is extensive or complex, consider including an anonymised genogram at the start of the chronology
Explain the background history of the victim and the perpetrator prior to the timescales under review stated in the terms of reference to give context to their story. Provide a combined narrative chronology charting relevant key events/contact/involvement with the victim, the perpetrator and their families by agencies, professionals and others who have contributed to the DHR process. Note the time and date of each occasion when the victim, perpetrator or child(ren) was seen and the views and wishes that were sought or expressed.
10. ANALYSIS
This part of the overview should examine how and why events occurred, information that was shared, the decisions that were made, and the actions that were taken or not taken. It can consider whether different decisions or actions may have led to a different course of events. The analysis section should address the terms of reference and the key lines of enquiry within them. It is also where any examples of good practice should be highlighted. The relevant research that underpins the analysis should be detailed.
Address each of the nine protected characteristics under the Equality Act 2010 and explain if they are relevant to the DHR. Include examining barriers to accessing services in addition to wider consideration as to whether service delivery was impacted. Additional vulnerabilities which may influenced access to services e.g. rural location
Analysis information required in the DHR and in the data collection
Aggravating Factors in the homicide including:
- Separation
- Coercive or controlling behaviour
- Stalking (physical / digital)
- Forced Marriage
- ‘Honour’-based abuse
- Faith-based abuse
- Sexual abuse
- Psychological or emotional abuse
- Physical abuse
- Economic abuse
Mental health issues identified for victim / perpetrator / children (both diagnosed and undiagnosed)
Vulnerabilities experienced by the victim and perpetrator:
- Experiencing alcohol misuse
- Experiencing other substance misuse
- Experiencing housing issues
- Physical disability
- Learning disabilities (including all diagnosed or undiagnosed neurodiversity)
- Speech, language and communication difficulties
- Pregnancy
- Mental ill-health
Previous abuse
- Had the victim been the victim of abuse previously
- Had the perpetrator previously been known to be a perpetrator of domestic abuse
- Has the victim/perpetrator been subject to adverse childhood experiences (ACEs)
Agency contact pertaining to the victim and perpetrator
- Any known contact with the police, probation or Children’s Social Services
- Had the victim been referred to MARAC at anytime
- Had the victim/perpetrator had contact with adult social care and/or mental health services
- Any known interaction/involvement with immigration
Children
- Were any children present when the death occurred
- Were any children subject to child protection procedures
- Were any children known to children’s social care
- If yes to the above, had referrals been made and then marked ‘no further action’
11. CONCLUSIONS
Bring together an overview of main issues identified and conclusions drawn from them which will translate into the detailing of lessons learnt in the next section.
12. LESSONS LEARNT AND RECOMMENDATIONS
This part of the DHR should summarise what lessons are to be drawn from the case and how those lessons should be translated into recommendations for action. State any early learning identified during the DHR process and whether this has already been acted upon.
Recommendations should include, but not be limited to, those made in Individual Management Reports and can include recommendations of national impact made for national level bodies or organisations. Recommendations should be focused and specific, timebound and implementable.
ANNEX A: DHR PROCESS
13. TIMESCALES
This DHR began on (date) and was concluded on (date). DHRs should be completed, where possible, within one year of the commencement. Explain any reasons for delay in completion.
14. CONTRIBUTORS TO THE DHR
- List the agencies and other contributors to the DHR and the nature of their contribution i.e. IMR, report, or information.
- Confirm the independence of IMR authors and how they are independent.
15. THE DHR PANEL MEMBERS
- List the agencies and roles of the panel members involved in the DHR Panel.
- Include number of times the DHR Panel met.
- Confirm independence of DHR Panel members.
- List sources of specialist advice where there was no representation amongst the DHR Panel. For example, economic abuse.
16. DHR AUTHOR
Explain the independence of the DHR Chair (and author if separate roles) and give details of their career history and relevant experience. Confirm that the DHR Chair/author have had no connection with the Community Safety Partnership. If they have worked for any agency in the area previously state how long ago that employment ended.
17. PARALLEL REVIEWS
State if an inquest or any other reviews or inquiries have been conducted and whether they have been used to inform this DHR.
18. SCOPING REVIEW
Attach the Scoping Review which was completed for this DHR.
Annex B: Action Plan Template and Guidance
Title of DHR
Governance arrangements: [Outline governance arrangements to oversee the implementation of DHR action plan]
| Recommendation | Action | Lead agency | Outcome that action will achieve | Responsible lead | Key milestones to complete action | Target date | Overall rag | Progress | Date of completion | Was outcome achieved? | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Recommendation | 1.1 Action | ||||||||||
| 1.2 Action | |||||||||||
| 1.3 Action | |||||||||||
| 1.4 Action | |||||||||||
| Recommendation | 2.1 Action | ||||||||||
| 2.2 Action | |||||||||||
| Recommendation | 3.1 Action | ||||||||||
| 3.2 Action |
Action Plan Guidance
Actions must be SMART:
- Specific
- Measurable
- Achievable
- Relevant
-
Time-bound
- Actions must be outcome focussed; this means the action plan must articulate what change can be expected as a result of the implementation of the action. For example, if the action identified is ‘x’ then the outcome might be ‘y’.
- Actions must have an identified responsible owner.
- As outlined in the section 18 of the DHR statutory guidance the CSP should agree future points that they will update family/friends on the implementation of the DHR Action Plan.
- During the development of the action plan the DHR Chair and local DHR Panel must engage with the relevant Police and Crime Commissioner to consider levers and governance for delivery of the action plan.
- The Domestic Abuse Commissioner will engage with CSPs to understand the progress of delivery of actions plans and be a point of escalation for instances where there are obstacles to implementation of actions or recommendations.
- When the final DHR is published the most up to date action plan should be added as an annex to the DHR with all implementation updates whilst noting that the action plan is a live document and is subject to change as outcomes are delivered. The CSP should publish the action plan on their own website and update as progress is made.
Annex C: Scoping Review Template
TITLE PAGE OF SCOPING REVIEW
- Name of the Community Safety Partnership
- Anonymised identifier as to which Scoping Review this refers to, i.e. pseudonym or number
- Date the Scoping Review was submitted to the Home Office
- Whether the CSP has commissioned a DHR or is recommending a DHR should not be commissioned
- Whether the death is a domestic homicide / neglect / suicide / still to be determined
-
How was the CSP notified of this death?
-
Summary of fatal incident
-
Background – what has been learnt about the victim and perpetrator?
-
What is the early learning that has been identified by agencies in this case?
-
What action(s), with outcomes and timelines will be taken as a result of the learning identified? [At this stage a comprehensive action plan is not necessary. Only actions already agreed at this stage need to be included. Actions identified in the Scoping Review should be automatically transferred to the DHR action plan as it is developed.]
-
If the Scoping Review Panel has agreed to not commission a DHR for this case please outline the rationale for this decision below.
-
What are the family/friends’ views on whether a DHR should be commissioned?
-
Which agencies and organisations have been consulted/involved in the Scoping Review?
-
Are there other reviews planned relating to this death?
Annex D: IMR Template
Name of person subject to review
Date of Birth
Date of Death
Job title and contact details of person completing this IMR (include confirmation regarding independence from the line management of the case).
INTRODUCTION
Brief factual/contextual summary of the situation leading to the DHR including an outline of the terms of reference and date for completion
VICTIM, PERPETRATOR, FAMILY DETAILS IF RELEVANT
| Name | Date of birth | Relationship | Ethnic origin | Address |
|---|---|---|---|---|
SUMMARY OF AGENCY INVOLVEMENT
- Construct a comprehensive chronology of involvement by your agency over the period of time set out in the review’s terms of reference.
- State when the victim/child/family/perpetrator was seen including antecedent history where relevant.
- Identify the details of the professionals from within your agency who were involved with the victim, family, perpetrator and whether they were interviewed or not for the purposes of this IMR.
- Include information on parallel reviews the agency is involved in.
ANALYSIS OF INVOLVEMENT
- Consider the events that occurred, the decisions made, and the actions taken or not.
- Assess practice against guidance, internal policies and relevant legislation.
- Provide details on any additional and relevant context.
ADDRESSING TERMS OF REFERENCE
Consider further analysis in respect of key critical factors, which are not otherwise covered by the sections above.
EFFECTIVE PRACTICE, LESSONS LEARNT & RECOMMENDATIONS
Recommendations should be focused on the key findings of the IMR and be specific about the outcome which they are seeking. This should also include details on recommendations that have already been actioned.
Annex E: Quality Assurance Board DHR feedback template
| Title of DHR | |
| Community safety partnership | |
| Date reviewed by GA board | |
| Decision | |
| Good practice commended |
| DHR SECTION | DHR QA BOARD FEEDBACK | ||
|---|---|---|---|
| Title Page | Improvements required before publication | ||
| Further improvements / notes for future DHRs | |||
| 1 | Contents Page | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 2 | Pen Portrait | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 3 | Condolences | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 4 | Confidentiality and Anonymity | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 5 | Terms of Reference | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 6 | Equality and Diversity | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 7 | Background Information | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 8 | Combined Chronology | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 9 | Overview | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 10 | Analysis | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 11 | Conclusions | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 12 | Lessons learnt and recommendations | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 13 | Timescales | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 14 | Involvement of family / friends / community | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 16 | DHR contributors | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 17 | DHR Panel | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 18 | DHR Author | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 19 | Parallel Reviews | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 20 | Dissemination | Improvements required before publication | |
| Further improvements / notes for future DHRs | |||
| 21 | Any other comments | Improvements required before publication | |
| Further improvements / notes for future DHRs |
Annex F: Equality and Diversity Toolkit
| Protected Characteristic | Prevalence |
|---|---|
| Age | Domestic abuse can happen at any age. Under section 3 of the Domestic Abuse Act 2021, children are now recognised as victims of domestic abuse in their own right, when they see, hear or experience the effects of domestic abuse and are related to either the perpetrator or victim, as victims of domestic abuse. The Crime Survey for England and Wales (CSEW) for the year ending March 2023 showed that a significantly higher proportion of people aged 16 to 19 years were victims of any domestic abuse (8.0%) compared with those aged 45 to 54 years (4.2%), and those aged 60 years and over (3.2% for 60 to 74 years). For those aged 75 years and over, the percentage of victims was significantly lower than all other age groups (1.4%). The Home Office Homicide Index shows that the average age of the 370 victims recorded between March 2020 – 2022 is 50. Just over a quarter (27.6%) of victims were 25 to 39 years old. A quarter (25.4%) were 65 or older.[footnote 18] |
| Disability | As defined by the Equality Act 2010, a person is disabled if they have a physical or mental impairment that has a ‘substantial’ and ‘long-term’ negative effect on your ability to do normal daily activities. Disabled people experience disproportionately higher rates of domestic abuse.[footnote 19] Specifically, the CSEW for year ending March 2023 found that adults aged 16 and over with disabilities are more than twice as likely to experience domestic abuse in the previous year (10.2%) than non-disabled adults (3.3%).[footnote 20] Of the 124 DHRs reviewed by the Home Office between October 2019 and October 2020, 12% of victims were recorded as having a physical disability and 5% had a recognised learning disability.[footnote 21] The 2021 census showed 17.8% of the population were considered disabled.[footnote 22] |
| Gender reassignment | Individuals who have undergone gender reassignment face specific types of abuse.[footnote 23] The CSEW for the year ending March 2023 shows that people aged 16 and over, who have had their gender reassigned since birth were over three times more likely to experience domestic abuse in the previous year (15.1%) in comparison to those who have not (4.4%)[footnote 24]. Data was collated on domestic abuse-related deaths – using a definition broader than the Domestic Abuse Act 2021 – by the Vulnerability Knowledge and Practice Programme (VKPP) between April 2020 - March 2022. None of the 470 victims were recorded as having undergone gender reassignment, although this characteristic was ‘not known’ or not recorded for 27% of victims.[footnote 25] |
| Marriage and civil partnership | For the year ending March 2023, the CSEW showed that a significantly larger proportion of adults aged 16 and over who were separated or divorced/in a legally dissolved partnership experienced domestic abuse in the previous year than those who were married or civil partnered, cohabiting, or widowed. However, marital status may have changed as a result of the abuse experienced.[footnote 26] |
| Pregnancy and maternity | Being pregnant may put women at increased risk of abuse, although the data available on prevalence of domestic abuse amongst pregnant individuals is limited. Some studies suggest as high as 40-60% of pregnant women experience abuse during pregnancy, while others suggest prevalence is much lower, ranging between 1% and 20%[footnote 27] (depending on the country and how prevalence is calculated)[footnote 28]. The 2020 – 2021 Home Office Domestic Homicide Review identified pregnancy as a vulnerability in 3 of 71 cases.[footnote 29] |
| Race & Ethnicity | The year ending March 2023 CSEW shows that adults aged 16 and over from a mixed ethnic background were more likely to have experienced domestic abuse within the previous year (7.9%) than those from white (4.7%), black (3.5%), or Asian or Asian British (2%) ethnic backgrounds. The Home Office Domestic Homicide Index finds that between March 2020 – 2022, 73.5% (272) of the 370 domestic homicide victims were white, 8.9% (33) were black and 14.9% (55) were of Other ethnic group.[footnote 30] The 2021 census highlights the overrepresentation of black ethnic groups in domestic abuse data; 81.7% of usual residents in England and Wales are white, 9.3% are Asian, Asian British or Asian Welsh, and 4% are black, black British, black Welsh, Caribbean, or African.[footnote 31] |
| Religion and belief | Victims who follow a religion or are from faith backgrounds may experience additional barriers to receiving help or reporting abuse due to issues with accessing support.[footnote 32] They might fear their faith being misunderstood or have concerns around whether they will be believed. In the year ending March 2023, adults aged 16 and over with no religion (5.3%), Other (5.2%). or Buddhist (5.1%) religion were most likely to report experiencing domestic abuse. This compares to 4.1% of Christians, 1.6% of Hindus and 1% of Muslims.[footnote 33] Understanding a victim’s religion or belief may provide useful context when conducting a DHR. The Home Office review of 124 domestic homicides between 2019 – 2020 asked whether religion was a ‘relevant factor’ in the case. There were no reviews where it was a relevant factor.[footnote 34] |
| Sex | Whilst both men and women can experience domestic abuse, statistics from 2023 CSEW highlight that women aged 16 and over are almost twice as likely to experience domestic abuse in the previous year than men (5.7% and 3.2% respectively). The 2020 – 2022 Home Office Homicide Index shows that 67.3% of the 370 domestic abuse victims were women, and 32.7% were male. In 88.6% of these cases, the suspects were male and in 11.4% they were female. For the majority (74.7%) of female domestic homicides, the suspect was a male partner or ex-partner, whereas in the majority (66.1%) of male domestic homicides, the suspect was a male family member.[footnote 35] This highlights the over representation of victims who are women in domestic homicide cases. |
| Sexual Orientation | LGBT victims can have a similar experience of domestic abuse to heterosexual victims, although they may face specific abusive behaviours relating to their sexual orientation.[footnote 36] CSEW data for the year ending March 2023 suggests that LGBT victims were more likely to report being victims of domestic abuse. 7.6% of gay men and lesbian women aged 16 and over were victims of domestic abuse in the previous year, as were 17.3% of bisexuals. This compares to 4% of heterosexual respondents.[footnote 37] With regards to their representation in domestic homicides, the data collated by the VKPP between April 2020 - March 2022 show that 16 of the 470 victims (3%) were recorded as being LGBTQ+. For 32% of victims this characteristic was listed as ‘not known’ or was not recorded, whilst it was recorded as ‘no’ for 64% of victims. Whilst the prevalence of LGB+ victims in domestic homicides matches the figure of LGB+ individuals recorded in the general population data[footnote 38], this figure is likely to be underreported due to barriers individuals may fear when disclosing their identity, and in turn lowering the level of engagement these victims may have with relevant support services.[footnote 39] |
Annex G: Involvement of family, friends, work colleagues, neighbours and wider community toolkit
| Action/Question | Answer | |
|---|---|---|
| 1 | What was the nature of the relationship of those involved in the DHR? Family, friends, work colleagues, neighbours or wider community | |
| 2 | First date contacted | |
| 3 | Nature of their involvement | |
| 4 | Was a Home Office leaflet provided? (Y/N) | |
| If no, why? | ||
| 5 | Was specialist advocacy offered? (Y/N) | |
| If no, why? | ||
| 6 | Have the Terms of Reference been shared? (Y/N) | |
| Was the opportunity to feedback on the Terms of Reference offered? (Y/N) | ||
| If no, why? | ||
| 7 | Date they met with the DHR Panel | |
| If they did not meet with the Panel, why? | ||
| 8 | Were they regularly updated on the progress of the DHR? (Y/N) | |
| State the regularity of updates | ||
| If they were not regularly updated, why? | ||
| 9 | Were they given the draft DHR to review and provide feedback before submission to the DHR QA Board? | |
| If no, why? | ||
| 10 | Were any adjustments made for their engagement? e.g. use of interpreters, or translation of DHR provided. |
Annex H: DHR Home Office Quality Assurance Board Terms of Reference
This Terms of Reference is subject to change. A full Terms of Reference will be developed and signed off by the QA Board Chair ahead of the publication of the DHR Statutory guidance.
1. Background
The Domestic Homicide Review (DHR) process is underpinned by the Domestic Violence, Crime and Victims Act 2004 which provides for local areas to carry out a DHR in instances where the death of a person aged 16 or over has, or appears to have, resulted from domestic abuse. It is held with a view to identifying the lessons to be learnt from the death.
The purpose of a DHR is to establish lessons learned regarding how local professionals and organisations work individually and together to safeguard victims. The DHR process helps to improve the response to domestic abuse and prevent future homicides. The Chair of the DHR identifies actions and makes recommendations for statutory agencies and Community Safety Partnerships (CSPs) to implement improved practices.
Quality assurance for completed DHRs rests with the expert board made of statutory and voluntary sector agencies and is manged by the Home Office.
2. Purpose
The purpose of the DHR Quality Assurance (QA) Board is to: ensure the DHR statutory guidance has been adhered to; that the DHR chair has engaged appropriate agencies, organisations and family and friends to establish as full a picture as possible; and that learning has been identified and the likelihood of further domestic abuse related deaths are minimised.
3. Responsibilities
The responsibilities of the QA Board are to:
- Review all DHRs submitted by the Home Office.
- Provide feedback on DHRs to CSPs and the DHR Chair, which is informed by the DHR statutory guidance and own professional expertise, this will include: the way that the review has followed the statutory guidance; the analysis of domestic abuse within the review; and the effectiveness and suitability of the recommendations that have been identified from the analysis of this fatality to prevent further domestic abuse.
- Identify areas of good practice within DHRs and where a DHR might need to be amended prior to publication.
- Share best practice and wider insight by publishing an annual report with data on DHRs reviewed and themes in QA Board feedback.
The QA Board’s responsibilities relate to England and Wales only and is not expected to provide ministerial advice on DHR issues, conduct media interviews on DHRs following publication, or respond publicly on DHRs.
Report Writer
- One non-statutory member will have the additional task of the annual report writer for the Chair.
- The DHR annual report is expected to include data on DHRs reviewed and themes in feedback and will be published online.
For QA Board members representing statutory organisations:
- Members will be required to review all the DHRs being considered by the QA Board, even where they may not cover their specific areas (e.g., policing, health, probation).
4. Membership and expertise
The Board members will consist of a mix of statutory and non-statutory members:
Members will need to demonstrate they have a minimum of 3 years’ experience gained in the public sector and/or voluntary sector or academia working on:
- domestic abuse or
- domestic homicide and/or suicide linked to domestic abuse
Chair and Secretariat
Chair: The Chair of the QA Board will be held by the Deputy Director, Home Office Interpersonal Abuse Unit and can be deputised to a Home Office official as needed.
What is expected from the Chair: The Chair will be expected to provide direction in bringing members to a consensus publication of individual DHR reports being considered at any given QA Board meeting.
Secretariat: The role of Secretariat will be held by officials within the Home Office Interpersonal Abuse Unit. Their function is to support the Board in delivering its remit. Tasks include, but are not limited to:
- Collating comments on DHRs from panel members
- Management of business plan/risk register and Board budget
- Support for data, analysis and policy development work
- Managing DHR thematic analyses and reviews
- Communications to board members
- Efficient management of the overall DHR Quality Assurance process
5. Standards for Members & Governance of Board Business
Members should at all times:
- Observe the highest standards of impartiality, integrity and objectivity in relation to the advice they provide and the management of the Board;
- Be accountable to the Home Office for its activities and for the standard of advice and decisions it makes;
- Act in accordance with the Seven Principles of Public Life: The Seven Principles of Public Life - GOV.UK (www.gov.uk);
- Comply with this code and ensure they understand their duties, rights and
- responsibilities and that they are familiar with the function and role of this body and any relevant statements of Government policy;
- Not misuse information gained in the course of their public service for personal gain or political purpose, nor seek to use the opportunity of public service to promote their private interests or those of connected persons, firms, businesses or other organisations;
- When engaging in other political activities, members should be conscious of their public role and exercise proper discretion.
6. Performance Management
The Chair should periodically review the performance of the Board, including the contribution, performance and conduct of individual members. Individual feedback should be provided to individual board members and in exceptional circumstances the Chair may submit advice to Home Office Ministers if satisfied that a Member;
(a) has become unfit or unable to discharge his or her functions properly, or
(b) has behaved in a way that is not compatible with continuing in their role.
7. Conduct of Meetings
Agenda
The following standard agenda shall be directed by the Chair:
-
A summary of each DHR to be considered will be read out by the Secretariat and then discussed by board members, who will have advance copies to read.
-
A vote will then take place by board members to decide based on the majority vote whether: the DHR can be published by the Community Safety Partnership (subject to feedback from the QA Board being reflected in the report); or if the DHR should be resubmitted to the QA Board for another QA check prior to publication.
Notice of Meetings
- The Secretariat will send the Board a Microsoft Teams meeting invite and provide all relevant DHR papers and agenda at least 1 month before the panel, and provide more time where permissible.
Frequency of meetings
- The normal frequency of the meeting will be monthly for 2 and half hours. However, the Chair can call additional meetings if needed and to ensure any backlog in DHRs are progressed in a timely manner.
8. Attendance
If for any reason board members are unable to attend the meeting under exceptional circumstances, then they should provide the QA Board with feedback on DHRs for consideration.
9. Escalation
There is no escalation process above the Chair of the QA Board should a Board member be dissatisfied for any reason.
10. Approval, review and variation of Terms of Reference Terms
The Secretary of State for the Home Department approves these Terms of Reference which can be reviewed and amended at any time.
Annex I: DHR Submission Checklist
Domestic Homicide Review Document Checklist for DHR Panel & CSP Use Prior to Submission of the DHR to the Home Office QA Board
This checklist is provided to assist DHR Panels and CSPs in their statutory sign off duties for their DHR with the aim of reducing the need for your DHR to be resubmitted due to missing information. Please use this checklist to ensure all information required as set out in the Statutory Guidance for the Conduct of Mult-Agency Domestic Homicide Reviews, Appendix 3 and 4, and the DHR Action Plan is covered in your DHR.
Please include this checklist with your DHR documents to the Home Office.
| Essential Information | ✔ Tick if Covered in DHR | |
|---|---|---|
| Title/ Contents Page | Contains: Name of CSP. Victim’s Pseudonym, month & year of death. DHR Chair/Author’s name. Date DHR completed. | |
| Has this been followed by a contents page? | ||
| Pen portrait | If the family have contributed a pen portrait of their family member, is this placed immediately after the contents page? | |
| Introductory paragraphs | A message of condolence has been included. | |
| Confidentiality | Confidentiality statement has been included | |
| The section contains the pseudonyms used to increase anonymity for the individuals involved and their families, and who chose the victim’s pseudonym, and who chose the perpetrator’s pseudonym is stated. Use of initials have been avoided. | ||
| Age of victim and perpetrator at the time of the fatal incident, and their ethnicity are included. | ||
| Terms of Reference | The key lines of enquiry (including sources of research) of the terms of reference are placed in the body of the DHR along with the time period the DHR is examining, and an explanation is given for the time period chosen to be reviewed. | |
| The key lines of enquiry contain case specific terms pertinent to the case, not just generic terms of reference. Where generic terms are included, these are included in the DHR and not just referenced. | ||
| The terms of reference may be relegated to an appendix. | ||
| Equality & Diversity | Have the nine protected characteristics under the Equality Act 2010 if relevant to the DHR have been fully explored? | |
| Have the characteristics and any diversity issues been examined to explore whether these were relevant to shaping the victim’s thinking about the decisions they made including barriers to accessing services | ||
| Did any of the protected characteristics impact on service delivery? | ||
| Were there any issues based on personal experience and needs to consider? | ||
| Did any of the subjects of the DHR have any specific vulnerabilities which impacted on the circumstances of the DHR? | ||
| Background Information (The Facts) | Has the following information required in guidance has been provided: Where the victim lived and where the homicide took place. A synopsis of the homicide (what actually happened and how the victim was killed is briefly described). | |
| Details of the Post Mortem and inquest and/or Coroner’s inquiry if already held. State the cause of death. | ||
| Members of the family and the household. Who else lived at the address or was a regular visitor and, if children were living there, what their ages were at the time (to enhance anonymity, the children’s sex should not be given in the DHR but should be provided in the Home Office data sheet). | ||
| How long the victim had been living with the perpetrator(s). If a partner/ex-partner, how long they had been together as a couple. | ||
| Who was charged with the homicide, the date (month & year), outcome of the trial, and sentence tariff? | ||
| If the DHR is being undertaken into a victim who died by suicide, on what basis this was considered to meet the criteria to undertake the DHR has been stated. | ||
| Chronology | Has the background history of the victim and the perpetrator prior to the timescales under review been included to give context to their story. | |
| A combined narrative chronology charting relevant key events/agency contact/involvement with the victim, the perpetrator and their families has been provided to show agency coordinated actions, or non-action. (Not an agency-by-agency report of contacts). The time (if available) and date of each occasion when the victim, perpetrator, or child(ren) were seen is included in the combined chronology and any views and wishes that were sought or expressed. | ||
| Overview | There is a summary of briefly describing information known to agencies and professionals about the victim, perpetrator, and their families. | |
| Any relevant facts or information about the victim and perpetrator. e.g. psychiatric report, or additional sources of information has been included, with identifying details removed. | ||
| Analysis | Has the Analysis addressed the Terms of Reference and/or key lines of enquiry within them? | |
| Has the Analysis adequately examined how and why events occurred, information that was shared, the decisions that were made, and the actions that were taken or not taken? | ||
| Has it considered whether different decisions or actions may have led to a different course of events? | ||
| Has the analysis been able to highlight any of good practice? | ||
| Have previous local DHRs been considered to check that agency deficits have been addressed? | ||
| Review practice the QA Board expect to see in a statutory report: Has the DHR used and cited suitable research to back up statements, to give examples of good practice, and to increase learning? | ||
| Conclusions | Have the Conclusion brought together an overview of main issues identified and are the key findings clearly expressed? | |
| Do the conclusions draw out issues which will translate into the lessons learnt in the next section? | ||
| If key agencies were not involved, has due consideration been given as to why this may be the case? | ||
| Has consideration been given as to what would need to be different about responses to achieve a different outcome? | ||
| Lessons to be Learnt | Has this section summarised what lessons are to be drawn from the case and how the lessons should be translated into recommendations for action? Are these lessons evidence based? | |
| Has any early learning identified during the DHR process been included? If so, has this included the date on which the early learning was acted upon and by whom? | ||
| Recommendations | Do the recommendations reflect the Lessons Learnt? | |
| Have IMR recommendations been included as expected? | ||
| Have any recommendations been made which could be of national impact and made for national level bodies or organisations? | ||
| Are the recommendations focused, specific, succinct, and capable of being implemented? |
| Annexes | Essential Information | ✔Tick if Covered in DHR |
|---|---|---|
| Timescales | Start and completion dates of the DHR are stated. | |
| Has an explanation for any delays in completion been stated? | ||
| Methodology | Have the following been included: Decision process to hold a DHR and who was involved, including if domestic abuse specialists were part of consultation process. | |
| When the Home Office and victim’s family were informed of the decision. | ||
| Methodology used, documents used, and any interviews undertaken. | ||
| Involvement of family, friends, colleagues, neighbours & wider community. | Have the following been included: When people were contacted and by whom. | |
| The nature of the individual’s involvement | ||
| Confirm provision of the Home Office DHR leaflet | ||
| The family had the help of a specialist and expert advocate. | ||
| The terms of reference were shared with them to assist with the scope of the DHR and what contribution the family made | ||
| The family met the DHR Panel and/or Chair | ||
| The family have been updated regularly | ||
| The family reviewed the draft DHR in private with plenty of time to do so and had the opportunity to comment and make amendments if required. | ||
| All those contributing were able to do so using the medium they prefer | ||
| Any changes or comments from the family are clearly recorded including any disagreements. | ||
| Contributors to the DHR | The names of agencies and other contributors and the nature of their contribution has been stated i.e. IMR, report, expert advice or other information, are listed. | |
| The independence of IMR authors has been confirmed. | ||
| The DHR Panel | The role, job title and the agency the Panel members represent are included. | |
| The independence of Panel members is stated. | ||
| The number of times Panel met is stated. | ||
| It is clear that the Panel is a mixture of statutory and voluntary sector agencies, and domestic abuse specialist services were Panel members. | ||
| Where an agency’s name does not clearly depict the service it provides the service has been explained in brackets or in a footnote. | ||
| The Author of the Overview Review Report | The independence of the DHR Chair & author (if separate roles) from the CSP and local agencies has been confirmed. | |
| Details of their career history and their relevant experience as per statutory guidance has been described | ||
| If they have worked for any agency previously the agency is named and when that employment ended has been included. | ||
| Parallel Reviews | State if an inquest or any other agency reviews or inquiries have been conducted and whether they have been used to inform this review. | |
| Dissemination | The dissemination list of recipients who will receive copies of the DHR are included, and the PCC has been included in the list to receive the DHR. | |
| Details are provided of any planned learning events or other methods of spreading the findings. |
The Action Plan
| Annexes | Essential Information | ✔Tick if Covered in DHR |
|---|---|---|
| The Action plan | Has your action plan used the template in statutory guidance or included all these headings in your plan? | |
| Do all the columns in your plan have the required text entered i.e. actions, lead agency name, the key milestone and target date? | ||
| Does your plan state clear outcomes expected to result from the recommendations in the Outcomes/Date Completed column? | ||
| If an action is marked completed, has the date of completion been inserted? | ||
| If all the actions to achieve a recommendation have been completed has the completion date been entered into the Outcome /Date completed column. |
Final Checks
| Proof Read Checks | Are the Contents Page list in the Overview and Executive Summary accurate? | |
|---|---|---|
| Does the Overview and Executive Summary include all the headings which appear in Appendix 3 and 4? | ||
| It is helpful to the QA Board and for feedback if the documents have paragraph numbers throughout. | ||
| Have the DHR documents been checked for typographical and formatting errors? | ||
| Where relevant, a glossary has been included? | ||
| Tone - Can you answer yes to the following questions? | If I were someone who loved the victim, would I think this DHR was open, honest and thorough? | |
| Have you ensured that proposed changes are focused on agencies changing rather than victims or their families? | ||
| Is the language used free of victim-blaming? | ||
| We need to learn about perpetrators behaviour and organisational interventions and opportunities with them. Has the DHR considered the perpetrator as a whole person, including the context of their background and history. |
Annex J: Domestic Homicide Review process maps
Figure 1: Domestic Homicide Review process map For further information on Domestic Homicide Review action plans, recommendation creation and implementation overview structures, please see Figure 3.
Figure 3: National and local oversight structures for DHR recommendations and actions.
Annex K: Glossary of Key Contacts
NHS England leads
| Region | |
|---|---|
| Midlands | [email protected] |
| East of England | [email protected] |
| London | [email protected] |
| Northeast and Yorkshire | [email protected] |
| Southwest | [email protected] |
| Southeast | [email protected] |
| Northwest | [email protected] |
CPS regional SPOC
For CPS SPOC, please find the relevant regional page on www.cps.gov.uk, and via the ‘contact us’ tab, submit a general enquiry for the attention (FAO) of the local Deputy Chief Crown Prosecutor (DCCP). They will then direct you to the current regional SPOC.
Home Office
| Role | |
|---|---|
| DHR Enquiries (Home Office) | [email protected] |
Domestic Abuse Commissioner
| Role | |
|---|---|
| DHR Inbox (DAC) | [email protected] |
Help and Support contacts
For links to online forms and webchat services, please click here: Domestic abuse: how to get help - GOV.UK (www.gov.uk)
| Nation | Helpline | Contact |
|---|---|---|
| England | Refuge’s National Domestic Abuse Helpline | 0808 2000 247 |
| Northern Ireland | Domestic and Sexual Abuse Helpline | 0808 802 1414 [email protected] |
| Scotland | Domestic Abuse and Forced Marriage Helpline | 0800 027 1234 [email protected] |
| Wales | Live Fear Free | 0808 80 10 800 [email protected] |
| UK-Wide | Men’s Advice Line | 0808 801 0327 [email protected] |
Homicide specific support
| Organisation | Contact |
|---|---|
| AAFDA (Advocacy After Fatal Domestic Abuse) | 07768 386922 www.aafda.org.uk |
| National Homicide Service | 0845 3030 900 www.victimsupport.org.uk |
Employers
| Organisation | Contact |
|---|---|
| EIDA (Employers’ Initiative on Domestic Abuse) | www.eida.org.uk |
| Refuge | 020 7395 7700 [email protected] |
| Respect | 020 7549 0578 [email protected] |
-
Mullane, F. (2017) ‘The impact of family members’ involvement in the domestic violence death review process’, in Dawson, M. (ed.) Domestic homicides and death reviews: an international perspective. London: Palgrave Macmillan, pp. 257–286. ↩
-
We acknowledge that in some circumstances a DHR may take place whilst the cause of death is still ‘suspected suicide’. However, for the purpose of this statutory guidance we will refer to all suspected and confirmed suicides as ‘died by suicide’. ↩
-
As defined in the Domestic Abuse Act 2021, a behaviour is “abusive” if it consists of physical or sexual abuse, violent or threatening behaviour, controlling or coercive behaviour, economic abuse, psychological, emotional or other abuse. ↩
-
Outlined in Chapter 1: Section 4 of the Equalities Act (2010), protected characteristics include: age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex and sexual orientation. ↩
-
To be referred to as ‘the QA Board’ from this point onwards. ↩
-
When referring to the VAWG specialist sector, this includes organisations that support male victims of these crimes also. ↩
-
Home Office. Violence against women and girls national statement of expectations: 2022 ↩
-
Further information on DHR Chair training will be provided at a later date. ↩
-
Colleagues in Wales should note Wales have an established trauma-Informed Wales Framework that should be referred to: Trauma-Informed Wales (traumaframeworkcymru.com) ↩
-
Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach: 2014. ↩
-
Research In Practice. Recognise and respond to trauma: 2023 ↩
-
WellPower. Language Matters When Talking About Suicide: 2019 ↩
-
A Pen Portrait is ‘a description of someone as a person (e.g. their personality, their likes and dislikes), their history (e.g. over their life course or more recently) as well as their needs or experiences’; Rowlands, J. (2020). ‘The ethics of victim voice in Domestic Homicide Reviews’. Sentio Journal. ↩
-
‘Communities’ includes colleagues, neighbours and anyone who may have had close and regular contact with the victim. ↩
-
Ministry of Justice and HM Prison and Probation Service. Probation Service Serious Further Offence procedures Policy Framework: 2021. ↩
-
Crown Prosecution Service. Disclosure Manual: 2022. ↩
-
For examples of cases where suicide has occurred following domestic abuse, see: [2018] EWCA Crim 690](https://www.bailii.org/cgi-bin/format.cgi?doc=/ew/cases/EWCA/Crim/2018/690.html&query=(Wallace)+AND+(.2018.)+AND+(EWCA)+AND+(Crim)+AND+(690)) and [2006] EWCA Crim 1139](https://www.bailii.org/cgi-bin/format.cgi?doc=/ew/cases/EWCA/Crim/2006/1139.html&query=(D)+AND+(.2006.)+AND+(EWCA)+AND+(Crim)+AND+(1139)). ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
Public Health England. Disability and domestic abuse: Risk, impacts and response. 2015 ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
Home Office. Key Findings from analysis of domestic homicide reviews: October 2019 to September 2020. 2021. ↩
-
ONS. Disability, England and Wales - Office for National Statistics (ons.gov.uk). Data year 2021. ↩
-
Harvey, S. et al. (2019). Barriers faced by lesbian, gay, bisexual and transgender People in Accessing Domestic Abuse, Stalking and Harassment, and Sexual Violence Services, Welsh Government. SafeLives. 2018. Free To be Safe: LGBT+ people experiencing domestic abuse. ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
Vulnerability Knowledge and Practice Programme (VKPP). Domestic Homicides and Suspected Victim Suicides 2021-2022, Year 2 Report: 2022. ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
Bailey B. A. (2010). Partner violence during pregnancy: prevalence, effects, screening, and management. International journal of women’s health, 2, 183–197. ↩
-
SafeLives. Cry for Health full report.pdf (safelives.org.uk) ↩
-
The smaller sample size represents a change in monitoring forms to collect this information. Home Office. 2022. Annex_A_DHRs_Review_Report_2020-2021.pdf (publishing.service.gov.uk) ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
ONS. Ethnic group, England and Wales: Census 2021. Data from 2021. ↩
-
Home Office. Domestic Abuse Act (2021) Statutory Guidance: 2022 ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
Home Office. 2022. Annex_A_DHRs_Review_Report_2020-2021.pdf (publishing.service.gov.uk) ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023. ↩
-
Home Office. Domestic Abuse Act (2021) Statutory Guidance: 2022 ↩
-
ONS. Domestic abuse victim characteristics, England and Wales - Office for National Statistics (ons.gov.uk). Data from year ending March 2023 ↩
-
ONS 2021 Census data shows that 3.2% of respondents identified with an LGB+ orientation. ONS. Sexual orientation, England and Wales - Office for National Statistics (ons.gov.uk). Data from 2021. ↩
-
See Spotlight #6: LGBT+ people and domestic abuse - Safelives ↩