Carbapenemase-producing Gram-negative organisms in England since October 2020: quarterly update, Q4 2023
Updated 23 December 2024
Applies to England

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/carbapenemase-producing-gram-negative-bacteria-laboratory-surveillance/carbapenemase-producing-gram-negative-organisms-in-england-since-october-2020-quarterly-update-q4-2023
Background
Since 1 October 2020, all diagnostic laboratories in England have a duty to notify the following via the UK Health Security Agency (UKHSA)’s Second Generation Surveillance System (SGSS) (1):
- acquired carbapenemase-producing Gram-negative organisms identified in human samples
- the results of any antimicrobial susceptibility test and carbapenem resistance mechanism in any of the causative agents listed in Schedule 2 of the Health Protection (Notification) Regulations 2020 (1).
This requirement was launched in conjunction with the national Framework of actions to contain carbapenemase-producing Enterobacterales (CPE), which sets out a range of measures that, if implemented well, will help health and social care providers minimise the impact of carbapenemase-producing organisms (CPO).
The analyses below are based on data relating to notifications of confirmed acquired CPOs between 1 October 2020 and 30 December 2023 in England. The data was extracted on 6 March 2024 from both UKHSA’s voluntary surveillance database, SGSS, and the Antimicrobial Resistance and Healthcare-Associated Infections (AMRHAI) Reference Unit database.
Rates of acquired CPOs were calculated using mid-year resident population estimates for the respective year and geography. Geographical analyses were based on the patient’s residential postcode. Where this information was unknown, the postcode of the patient’s GP was used. Failing that, the postcode of the reporting laboratory was used. Cases in England were further assigned to one of 9 local areas, formed from the administrative local authority boundaries.
As patients may have more than one positive specimen taken, specimens taken from the same patient that yielded growth of the same pathogen, carbapenemase and specimen type within a 52-week period from the initial positive specimen were regarded as comprising the same episode and were de-duplicated. Samples are split into three specimen types: sterile site specimens (eg blood or cerebrospinal fluid), screening site specimens (eg faeces or lower gastrointestinal tract) or ‘other’ specimen type (eg urine or lower genital tract). CPO referred isolates and local laboratory isolates were combined for this de-duplication process, with resistance mechanism results from the AMRHAI Reference Unit retained preferentially where patient specimen overlap occurred. (It should be noted that not all specimens in this report are confirmed by AMRHAI.) This method differs slightly from that of the weekly causative agent notification data where data is not de-duplicated incorporating specimen type. In addition, the data presented in the weekly notification reports utilises SGSS reports only.
The index of multiple deprivation (IMD) is a way of summarising the level of deprivation within an area, based on a set of factors that includes their levels of income, employment, education and local levels of crime. Episodes were linked to IMD using patient postcode (and GP or laboratory postcode where patient postcode was unavailable) and the IMD decile score was identified by the lower super output area the patient resided in.
The Office for Health Improvements and Disparities developed a method for assigning ethnic group based on hospital admissions data. As different ethnicities may be recorded in different treatment episodes, the method selected a single ethnic group from a patient’s HES records. Episodes were linked to ethnic group using patient NHS number and date of birth.
The following report summarises trends and geographical distribution of carbapenemase mechanisms identified from Gram-negative bacteria in human samples. Species, mechanism, sample type, and age and sex of patients are also described. For the purposes of this report, quarters are calendar quarters, as such January to March is referred to as ‘Q1’, April to June is referred to as ‘Q2’, July to September is referred to as ‘Q3’ and October to December is referred to as ‘Q4’, alongside relevant years.
Note: Scientific names are not italicised in this report to ensure our content is inclusive for all users and in compliance with web accessibility legislation and associated guidelines.
Microbiology services
For reference services, including species identification and confirmation of susceptibility testing results, laboratories should contact UKHSA’s Antimicrobial Resistance and Healthcare Associated Infections (AMRHAI) Reference Unit in Colindale, London.
Table 1 summarises the carbapenemase gene families that are targeted – using the routine polymerase chain reaction (PCR) applied to referred Enterobacterales, Pseudomonas spp. and Acinetobacter spp. – because they are suspected of harbouring an acquired carbapenemase gene. UKHSA strongly recommends that all diagnostic laboratories are able to detect, at least, the 4 carbapenemase families shown in bold in this table (the ‘big 4’) using either PCR or immunochromatographic methods.
Where an ‘exceptional’ carbapenemase and species combination result (cells without a ¥ symbol in Table 1) has been identified, or where an unusual organism has been identified with an acquired carbapenemase (that is, any bacterial genera other than a member of the Enterobacterales, Pseudomonas spp. or Acinetobacter spp.), isolates should be sent to the AMRHAI Reference Unit for confirmation.
Table 1. Distribution of carbapenemase genes covered by AMRHAI Reference Unit molecular assay (based on AMRHAI data) [note 1]
| Carbapenemase family | Associated with common ‘host’ organism Enterobacterales | Associated common ‘host’ organism Pseudomonas spp. | Associated with common ‘host’ organism Acinetobacter spp. |
|---|---|---|---|
| KPC | ¥ | <10D | <10D |
| OXA-48-like | ¥ | <10D | 0 |
| NDM | ¥ | ¥ | ¥ |
| VIM | ¥ | ¥ | <10D |
| IMP | ¥ | ¥ | ¥ |
| IMI/NMC-A | ¥B | 0 | 0 |
| GES | ¥ | ¥ | <10D |
| FRI | <10 | 0 | 0 |
| SME | ¥C | 0 | 0 |
| DIM | 0 | <10D | 0 |
| GIM | <10D | <10D | 0 |
| SIM | 0 | <10D | 0 |
| SPM | 0 | <10D | 0 |
| OXA-23-like | <10D | 0 | ¥ |
| OXA-40-like | 0 | 0 | ¥ |
| OXA-51-likeA | 0 | 0 | ¥ |
| OXA-58-like | 0 | 0 | ¥ |
View this table in the data tables file
Notes to Table 1
Note 1. Table 1 uses the following symbols:
¥ = combinations of mechanism and species would not be considered as exceptional results.
A = intrinsic to A. baumannii and only expressed when associated with an insertion element.
B = almost exclusively reported in Enterobacter spp. with less than a handful of reports in other genera.
C = reported only in Serratia marcescens.
D = fewer than 10 in total ever referred to AMRHAI Reference Unit.
Recent developments
Unusual acquired CPOs referred to the AMRHAI Reference Unit in Q4 2023 consisted of one isolate of Aeromonas caviae positive for a blaOXA-48-like gene from an environmental sample in the North West. Carbapenem resistance in Aeromonas spp. is usually mediated by a chromosomal cphA gene, which confers a metallo-carbapenemase-like phenotype, but occasionally transmissible carbapenemase genes belonging to the ‘big 5’ families have been identified (2). The AMRHAI Reference Unit does not currently seek carbapenem-resistant Aeromonas spp. unless there is reason to suspect they are carrying an acquired carbapenemase gene. A rectal swab isolate of Klebsiella pneumoniae ST258 producing a KPC enzyme with the D179Y amino acid substitution that confers resistance to ceftazidime/avibactam (3) was referred by a London laboratory; this is only the second such isolate that AMRHAI have identified amongst submissions since PCR screening was introduced in 2019. A further two Proteus mirabilis isolates carrying a blaOXA-23 carbapenemase gene were referred by laboratories in the South East and London from a urine sample and a rectal swab; sequencing analysis is being undertaken to compare these with the previous isolates referred to AMRHAI and with the OXA-23-producing P. mirabilis clone reported in France and Belgium.
Locally-confirmed unusual combinations of organism and mechanism should be referred to the AMRHAI Reference Unit for confirmation. Follow up of these unusual combinations has identified some isolates have been due to mixed cultures or reporting errors.
Specimen type
Between October 2020 and December 2023, there were 13,126 acquired CPO episodes reported. The majority were identified in screening samples, accounting for 71.9% of notifications, with only 4.5% reported in sterile site specimens (Table 2).
Table 2. Number and percentage of acquired CPO episodes by specimen type (England): October 2020 to December 2023
| Specimen type | All reports number | All reports % [note 3] | From AMRHAI number | From AMRHAI % [note 4] |
|---|---|---|---|---|
| Sterile site samples | 597 | 4.5 | 215 | 10.8 |
| Screening samples | 9,432 | 71.9 | 940 | 47.2 |
| Other samples [note 2] | 3,097 | 23.6 | 838 | 42.0 |
| All samples | 13,126 | 100.0 | 1,993 | 100.0 |
View this table in the data tables file
Notes to Table 2
Note 2. Samples that do not fall into either ‘sterile site’ or ‘screening’ samples, for example, urine and lower genital tract specimens.
Note 3. The percentages presented in this table are column percentages, with the breakdown of specimen types shown for all reports and AMRHAI reports separately.
Note 4. The AMRHAI Reference Unit actively encourages submission of sterile site isolates for carbapenemase confirmation; the distribution of specimen type will reflect this.
Quarterly trends
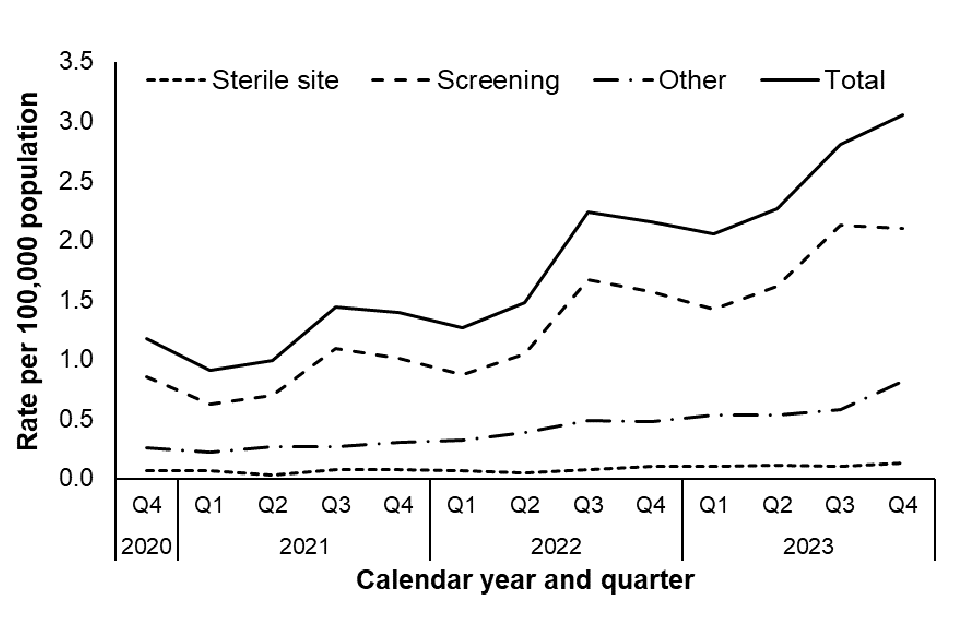
The quarterly rate of acquired CPO episodes between October 2020 and December 2023 is shown in Figure 1.
Although in this quarter the rate of CPO episodes continues to increase, from 2.8 per 100,000 population in Q3 2023 to 3.1 per 100,000 population in Q4 2023, this rise was predominantly due to increases in rates among ‘other’ sample types, and a small increase in the rate sterile site isolates (Figure 1). The rate of CPO episodes from screening isolates remained stable in Q4 compared to Q3 of 2023; however this rate represents a higher rate of episodes compared to quarters prior to Q3 2023.
It is important to note that quarterly changes in rate of episodes may reflect an uptick in screening following changes to screening policy and/or an improvement in national reporting of CPO episodes rather than an actual increase in incidence. Furthermore, as there are only 13 quarters of notification data, it is too early to conclude that there may be any seasonality, particularly in light of the COVID-19 pandemic, where quarterly changes may be affected by the COVID-19 pandemic during this period or associated with local CPO outbreaks.
The remaining data summaries in this report consider all samples grouped together, except Table 4.
Figure 1. Rate of acquired CPO episodes by specimen type and quarter (England): October 2020 to December 2023
Geographic distribution
The rate of acquired CPO episodes varied by Office for National Statistics (ONS) region (Figure 2), with the highest overall rate between January 2023 and December 2023 reported in London (2.4 episodes per 100,000 population), followed by the North West (2.2 episodes per 100,000 population). The lowest incidence across the last year was reported in the South West region (0.2 per 100,000 population).
Figure 2. Geographical distribution of acquired CPO incidence rates per 100,000 population (England): January 2023 to December 2023 [note 5]

Notes to Figure 2
Note 5. The region geography is based on the laboratory location and linked to the ONS data for regions.
The number and rate of reported acquired CPO episodes for each ONS region by calendar quarter is shown in Table 3.
The rate of bacterial episodes in all ONS regions increased from Q3 2023 to Q4 2023 in all regions except London and the North East, where the rates decreased (but still remained above the reported rates in Q1 and Q2). The rate in the South East nearly doubled (0.8 to 1.5 per 100,000 population) and the the rate for Yorkshire and Humber increased by a third (1.7 to 2.4 per 100,000 population).
Table 3. Number of acquired CPO episodes and rate per 100,000 population by ONS region (England): January 2023 to December 2023
| ONS region | Q1 number | Q1 rate | Q2 number | Q2 rate | Q3 number | Q3 rate | Q4 number | Q4 rate |
|---|---|---|---|---|---|---|---|---|
| East Midlands | 48 | 1.0 | 46 | 0.9 | 51 | 1.0 | 69 | 1.4 |
| East of England | 25 | 0.4 | 33 | 0.5 | 55 | 0.9 | 71 | 1.1 |
| London | 438 | 5.0 | 450 | 5.1 | 522 | 5.9 | 478 | 5.4 |
| North East | 57 | 2.2 | 38 | 1.4 | 101 | 3.8 | 92 | 3.5 |
| North West | 310 | 4.2 | 349 | 4.7 | 404 | 5.4 | 422 | 5.7 |
| South East | 63 | 0.7 | 71 | 0.8 | 75 | 0.8 | 138 | 1.5 |
| South West | 16 | 0.3 | 17 | 0.3 | 34 | 0.6 | 37 | 0.6 |
| West Midlands | 132 | 2.2 | 200 | 3.4 | 253 | 4.3 | 284 | 4.8 |
| Yorkshire and The Humber | 74 | 1.4 | 74 | 1.4 | 93 | 1.7 | 133 | 2.4 |
View this table in the data tables file
The number of acquired CPO episodes for each ONS region by calendar quarter and specimen type is shown in Table 4.
London had the highest percentage of bacterial episodes reported in sterile site specimens and screening samples across all four quarters (Q1 2023 – Q4 2023) compared to other regions, whereas the North West had the highest percentage of bacterial episodes reported in other samples, replacing London, for Q4 2023. An increase from 5.0% in Q3 2023 to 17.3% in Q4 2023 in sterile site specimens was noted in the South East, comprising an additional 10 sterile site samples reported in Q4 compared to Q3 (Table 4) – this increase is being investigated further.
Table 4. Percentage of acquired CPO episodes by ONS region and specimen type (England): January 2023 to December 2023
| ONS region | Q1 Sterile site % | Q2 Sterile site % | Q3 Sterile site % | Q4 Sterile site % | Q1 Screening % | Q2 Screening % | Q3 Screening % | Q4 Screening % | Q1 Other % [note 1] | Q2 Other % [note 1] | Q3 Other % [note 1] | Q4 Other % [note 1] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| East Midlands | 5.1 | 3.1 | 5.0 | 6.7 | 4.4 | 3.0 | 2.9 | 3.9 | 3.3 | 5.6 | 4.0 | 3.9 | |
| East of England | 1.7 | 4.7 | 10.0 | 16.0 | 1.0 | 1.0 | 1.3 | 2.0 | 5.3 | 6.9 | 10.4 | 7.6 | |
| London | 44.1 | 45.3 | 53.3 | 34.7 | 37.3 | 33.5 | 33.0 | 26.7 | 37.4 | 38.3 | 28.7 | 29.3 | |
| North East | 6.8 | 1.6 | 3.3 | 0.0 | 4.6 | 3.3 | 7.1 | 7.0 | 5.3 | 2.3 | 4.3 | 2.0 | |
| North West | 18.6 | 15.6 | 3.3 | 9.3 | 31.5 | 32.3 | 29.8 | 23.3 | 15.2 | 14.9 | 13.4 | 29.9 | |
| South East | 6.8 | 3.1 | 5.0 | 17.3 | 4.4 | 4.1 | 3.4 | 7.0 | 7.9 | 10.6 | 9.5 | 9.1 | |
| South West | 3.4 | 3.1 | 1.7 | 1.3 | 0.7 | 1.2 | 1.8 | 2.2 | 2.6 | 1.3 | 3.4 | 2.2 | |
| West Midlands | 10.2 | 9.4 | 10.0 | 10.7 | 10.2 | 16.6 | 15.7 | 19.8 | 14.6 | 14.2 | 18.0 | 8.9 | |
| Yorkshire and The Humber | 3.4 | 14.1 | 8.3 | 4.0 | 5.9 | 5.2 | 5.0 | 8.2 | 8.3 | 5.9 | 8.5 | 7.2 |
Notes to Table 4
Note 1. Samples that do not fall into either ‘sterile site’ or ‘screening’ samples, for example, urine and lower genital tract specimens.
Geographical differences in carbapenemase family
Between January 2023 and December 2023, the most common carbapenemase families reported across all regions were NDM (34.8%), OXA-48-like (34.1%) and KPC (22.8%). However, the distribution of carbapenemase families identified varied regionally (Figure 3).
In London, which had the highest incidence rate, the most commonly reported carbapenemase families identified were NDM (47.0%) and OXA-48-like (38.4%). However, in the North West, which also had a high incidence rate, KPC accounted for 49.2% of episodes. KPC was not as common in any of the other regions, accounting for fewer than 31.9% of episodes in each region; in London, KPC accounted for 4.3% of episodes.
Another regional difference was observed in the North East and Yorkshire and the Humber, where IMP was more commonly reported compared to any of the other regions, accounting for 16.0% and 11.0% of episodes, respectively (other regions reporting fewer than 8.6%). However, given the small number of carbapenemases reported in some regions, the diversity of carbapenemases reported is likely to be strongly impacted by individual outbreaks. In the two regions that had the lowest incidence rates, the most common carbapenemase family was OXA-48-like (60.3% in the East of England and 45.2% in the South West).
The distribution of carbapenemase families within each ONS region also varied by quarter. For example, the most commonly reported carbapenemase family identified in the West Midlands was predominantly OXA-48-like in Q4 2023 (57.4%) but in Q1 2023 it was predominantly KPC (37.1%).
Figure 3. Geographical distribution of acquired CPO episodes by carbapenemase family (England): January 2023 to December 2023

Notes to Figure 3
Note 6. Other carbapenemase families include DIM, GES, GIM, IMI, OXA-23 (in genera other than Acinetobacter spp.).
Distribution of species and carbapenemase family
Between January 2023 and December 2023, the most frequently isolated Gram-negative bacterial species with a confirmed acquired CPO was Escherichia coli, accounting for 33.3% of all specimens. This was followed by Klebsiella pneumoniae, and Enterobacter spp., which accounted for 31.2% and 18.8% of all specimens, respectively (Table 5).
The carbapenemase family most frequently identified in E. coli and K. pneumoniae isolates was OXA-48-like (41.8% and 35.3%, respectively). In Enterobacter spp. isolates this was NDM (39.5%), followed by KPC and OXA-48-like carbapenemase families (22.9% and 20.6%, respectively). In E. coli the mechanisms most commonly reported after OXA-48-like were NDM and KPC (41.7% and 13.8%, respectively), and in K. pneumoniae isolates KPC and NDM carbapenemase families (30.4% and 29.3%, respectively).
Aside from the ‘big 5’ carbapenemase families (KPC, OXA-48-like, NDM, VIM and IMP), the AMRHAI Reference Unit also screens for rarer carbapenemase families, and it is recommended that all isolates suspected to produce an acquired carbapenemase but are negative for the ‘big 5’ carbapenemase families are referred to the AMRHAI Reference Unit for further testing. Between October 2020 and December 2023, DIM, GES, GIM, IMI, OXA-23 and SME carbapenemases were identified in small numbers (1, 29, 8, 34, 8 and 2, respectively), with only five isolates (GIM positive) being identified from invasive specimens.
Table 5. Acquired CPO episodes by species and carbapenemase family (England): January 2023 to December 2023
| Species | IMP number (%) | KPC number (%) | NDM number (%) | OXA-48-like number (%) | VIM number (%) | Other number (%) | Total number | % of Total per species |
|---|---|---|---|---|---|---|---|---|
| Acinetobacter spp. [note 7] | 6 (10.7) | 1 (1.8) | 45 (80.4) | 2 (3.6) | 2 (3.6) | 0 (0.0) | 56 | 1.0 |
| Citrobacter spp. | 13 (4.4) | 72 (24.3) | 64 (21.6) | 133 (44.9) | 13 (4.4) | 1 (0.3) | 296 | 5.1 |
| Enterobacter spp. | 144 (13.3) | 247 (22.9) | 426 (39.5) | 222 (20.6) | 31 (2.9) | 9 (0.8) | 1,079 | 18.8 |
| Escherichia coli | 35 (1.8) | 265 (13.8) | 799 (41.7) | 800 (41.8) | 16 (0.8) | 0 (0.0) | 1,915 | 33.3 |
| Other Escherichia spp. | 2 (13.3) | 10 (66.7) | 2 (13.3) | 1 (6.7) | 0 (0.0) | 0 (0.0) | 15 | 0.3 |
| Klebsiella oxytoca | 4 (2.1) | 102 (54.0) | 17 (9.0) | 61 (32.3) | 5 (2.6) | 0 (0.0) | 189 | 3.3 |
| Klebsiella pneumoniae | 41 (2.3) | 547 (30.4) | 527 (29.3) | 635 (35.3) | 46 (2.6) | 1 (0.1) | 1,797 | 31.2 |
| Other Klebsiella spp. | 4 (5.0) | 20 (25.0) | 17 (21.3) | 37 (46.3) | 2 (2.5) | 0 (0.0) | 80 | 1.4 |
| Morganella spp. | 0 (0.0) | 1 (6.3) | 4 (25.0) | 9 (56.3) | 2 (12.5) | 0 (0.0) | 16 | 0.3 |
| Pseudomonas aeruginosa [note 7] | 19 (13.9) | 3 (2.2) | 53 (38.7) | 6 (4.4) | 48 (35.0) | 8 (5.8) | 137 | 2.4 |
| Other Pseudomonas spp. [note 7] | 0 (0.0) | 1 (3.7) | 9 (33.3) | 0 (0.0) | 17 (63.0) | 0 (0.0) | 27 | 0.5 |
| Serratia spp. | 0 (0.0) | 0 (0.0) | 9 (33.3) | 18 (66.7) | 0 (0.0) | 0 (0.0) | 27 | 0.5 |
| Other Enterobacterales [note 8] | 4 (3.4) | 42 (36.2) | 31 (26.7) | 37 (31.9) | 2 (1.7) | 0 (0.0) | 116 | 2.0 |
| Other Gram-negative bacteria [note 9] | 1 (50.0) | 0 (0.0) | 1 (50.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 | 0.0 |
| Total | 273 (4.7) | 1311 (22.8) | 2004 (34.8) | 1961 (34.1) | 184 (3.2) | 19 (0.3) | 5,752 | 100.0 |
View this table in the data tables file
Notes to Table 5
Note 7. KPC and OXA-48-like in Pseudomonas spp. and OXA-48-like in Acinetobacter spp. are extremely rare, and results should be interpreted with caution. The numbers reported here have not all been confirmed by the AMRHAI Reference Unit and laboratories identifying these unusual combinations should be referring such isolates to AMRHAI.
Note 8. Includes coliform, Cronobacter spp., Hafnia spp., Kluyvera spp., Leclercia adecarboxylata, Lelliottia amnigena, Mixta calida, Pantoea spp., Phytobacter ursingii, Pluralibacter gergoviae, Proteus spp., Providencia spp., Raoultella spp., and Shigella spp.
Note 9. The numbers reported here have not all been confirmed by the AMRHAI Reference Unit and laboratories identifying these unusual combinations should be referring such isolates to AMRHAI.
Distribution of demographic risk factors
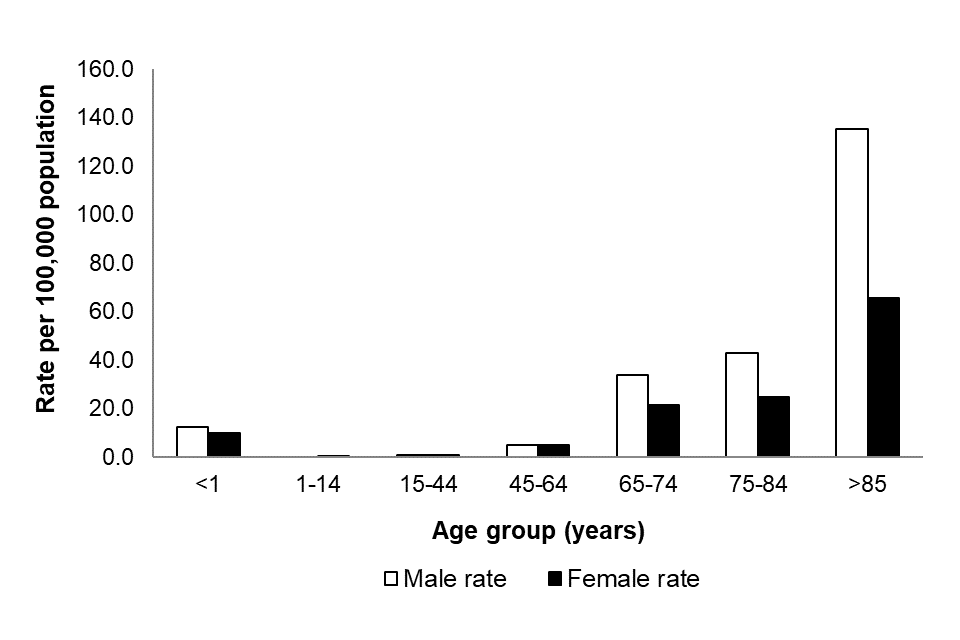
Between January 2023 to December 2023, the rate of reported acquired CPO episodes was highest among the oldest and youngest members of the population. A similar age pattern was noted for both sexes, although overall the rate was higher in males compared to females (overall rates of 9.9 and 7.4 episodes per 100,000 population, respectively: Figure 4). This aligns with the age group and sex distribution noted in previously published reports on Gram-negative bacteraemia such as E. coli, Klebsiella spp., P. aeruginosa and Enterobacter spp.
Figure 4 shows the reported acquired CPO incidence rates by age group between January 2023 to December 2023, with the highest rate reported in those 85 years and over (91.6 per 100,000 population) followed by those aged 75-84 years (33.0 per 100,000 population). The overall rate of confirmed CPOs was 11.2 per 100,000 population in infants less than one year old.
Figure 4. Rate [note 10] of acquired CPO episodes per 100,000 population by age and sex [note 11] (England): January 2023 to December 2023
Notes to Figure 4
Note 10. Rates have been calculated using cumulative reports across the last 4 quarters of reporting and, as such, cannot be compared to previous quarters (4).
Note 11. Information about patient sex is only recorded in 99.4% of cases.
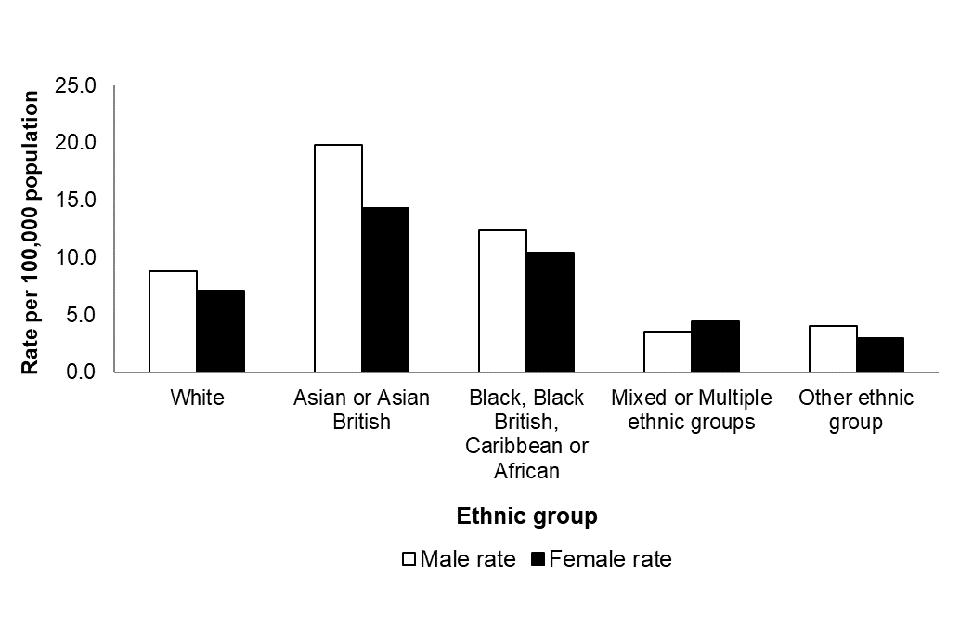
Figure 5. Rate [note 10] of acquired CPO episodes per 100,000 population by sex [note 11] and ethnic group [note 12] (England): January 2023 to December 2023
Notes to Figure 5
Note 10. Rates have been calculated using cumulative reports across the last four quarters of reporting, and as such cannot be compared to previous quarters (4).
Note 11. Information about patient sex is only recorded in 99.4% of cases.
Note 12. Information about patient ethnicity in only recorded in 89.5% of cases.
Between January 2023 and December 2023, the most common carbapenemase families reported across all ethnic groups were OXA-48-like (34.6%), NDM (32.5%), and KPC (24.6%) (Figure 6). Similar to regional distribution, the distribution of carbapenemase families identified also varied across ethnic groups. In those of Asian or Asian British ethnicity, who had the highest incidence rate, the most common carbapenemase families identified were NDM (56.9%) and OXA-48-like (32.9%). KPC was not as common in those of Asian or Asian British ethnicity (7.3%) however in those of White ethnicity, KPC accounted for 30.0% of episodes.
Figure 6. Distribution of acquired CPO episodes by ethnic group [note 12] and carbapenemase family (England): January 2023 to December 2023

Notes to Figure 6
Note 6. Other carbapenemase families include DIM, GES, GIM, IMI and OXA-23 (in genera other than Acinetobacter spp.).
Note 12. Information about patient ethnicity in only recorded in 89.5% of cases.
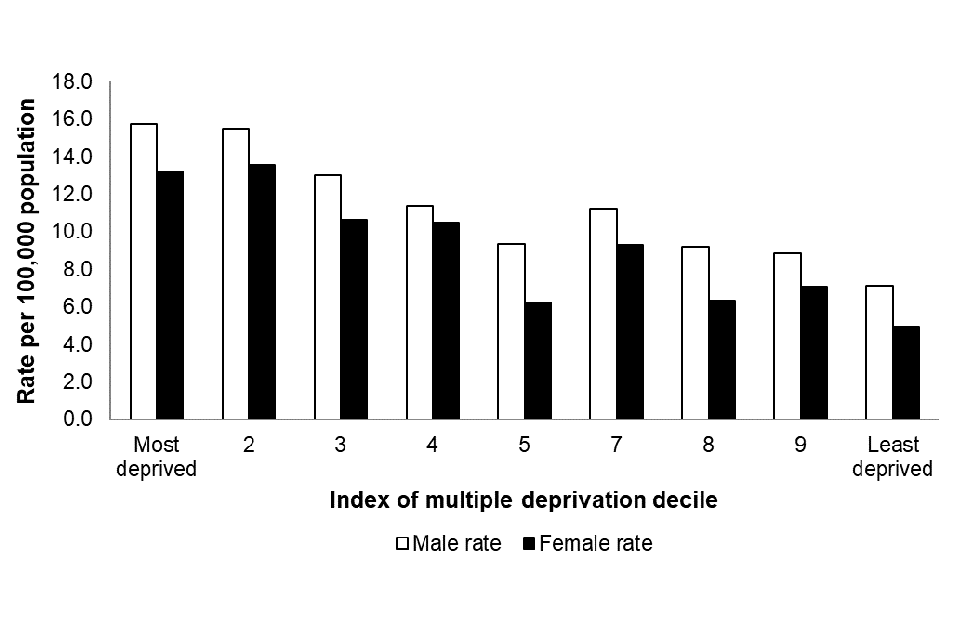
Figure 7 shows the acquired CPO incidence rates by IMD decile and sex between January 2023 to December 2023. The highest rate was reported in those in the bottom two (most deprived) deciles (both 14.5 per 100,000 population). The rate generally declines as the IMD decile increases, with the lowest rate reported in the least deprived IMD decile (6.0 per 100,000 population). A similar pattern was noted for both sexes, although overall the rate was higher in males compared to females (overall rates of 7.1 and 4.9 episodes per 100,000 population, respectively).
Figure 7. Rate [note 10] of acquired CPO episodes per 100,000 population by index of multiple deprivation decile and sex [note 11] (England): January 2023 to December 2023
Notes to Figure 7
Note 10. Rates have been calculated using cumulative reports across the last four quarters of reporting, and as such cannot be compared to previous quarters (4).
Note 11. Information about patient sex is only recorded in 99.4% of cases.
Figure 8 shows the acquired CPO incidence rates by IMD decile and carbapenemase family between January 2023 to December 2023. The three carbapenemase families with the highest rates across all IMD deciles are OXA-48-like, KPC and NDM, where the rate generally declines with increasing IMD decile (least deprived); for example, the rate for OXA-48-like is 4.4 per 100,000 for the most deprived IMD decile and declines to 1.8 per 100,000 for the least deprived IMD decile.
Figure 8. Rate [note 10] of acquired CPO episodes per 100,000 population by index of multiple deprivation decile and resistance mechanism (England): January 2023 to December 2023

Notes to Figure 8
Note 6. Other carbapenemase families include DIM, GES, GIM, IMI and OXA-23 (in genera other than Acinetobacter spp.).
Note 10. Rates have been calculated using cumulative reports across the last four quarters of reporting, and as such cannot be compared to previous quarters (4).
Quarterly mandatory laboratory return reporting (January 2023 to December 2023)
Table 6. Quarterly mandatory laboratory returns (QMLR) for the total number of rectal swabs and faecal screening specimens taken for CPO screening by acute trust type [note 13] (England): January 2023 to December 2023
| Trust type [note 13] | Q1 2023 reported screens (%) | Q1 2023 total screens | Q2 2023 reported screens (%) | Q2 2023 total screens | Q3 2023 reported screens (%) | Q3 2023 total screens | Q4 2023 reported screens (%) | Q4 2023 total screens |
|---|---|---|---|---|---|---|---|---|
| Small (n=21) | 13 (61.9) | 5,783 | 14 (66.7) | 5,209 | 13 (61.9) | 6,542 | 12 (57.1) | 5,421 |
| Medium (n=21) | 19 (90.5) | 7,051 | 18 (85.7) | 6,741 | 17 (81.0) | 7,017 | 14 (66.7) | 5,293 |
| Large (n=24) | 19 (79.2) | 11,980 | 19 (79.2) | 14,010 | 18 (75.0) | 18,357 | 18 (75.0) | 20,046 |
| Multi-service (n=7) | 7 (100.0) | 2,219 | 7 (100.0) | 3,079 | 7 (100.0) | 6,291 | 4 (57.1) | 6,654 |
| Specialist (n=16) | 11 (68.8) | 4,196 | 11 (68.8) | 4,441 | 11 (68.8) | 4,073 | 11 (68.8) | 4,225 |
| Teaching (n=48) | 38 (79.2) | 70,714 | 36 (75.0) | 72,829 | 37 (77.1) | 78,715 | 32 (66.7) | 58,550 |
| Total (n=137) | 107 (78.1) | 101,943 | 105 (76.6) | 106,309 | 103 (75.2) | 120,995 | 91 (66.4) | 100,189 |
View this table in the data tables file
Notes to Table 6
Note 13. Trust type obtained through NHS Digital Estate Return Information Collection (ERIC).
Reporting of quarterly totals of rectal swabs and faecal specimens taken for CPO screening was added to the mandatory quarterly laboratory returns (QMLR) section of the HCAI DCS in October 2019, and reporting became mandatory in October 2020. Between January 2023 to December 2023, there were 429,436 screens reported by 108 NHS Trusts leading to an overall Trust reporting rate of 78.8% (Table 5). Of the acute Trusts that reported at least 1 screening report between January 2023 to December 2023, 4.6% reported that they conducted zero screens and 26.9% did not submit a return.
Between January 2023 to December 2023, the number of Trusts that reported screens declined from 78.1% to 66.4%. Reported screening was more predominant in the acute teaching Trusts, accounting for 65.4% of screening swabs taken during this time period. By reporting acute Trust, the total screens reported for the past four quarters ranged from 0 to 19,078. The full list of reporting, including those that did not submit a return, is available in the data appendix by individual NHS acute Trust.
References
1. Department of Health and Social Care (2020). The Health Protection (Notification) (Amendment) (No.2) Regulations 2020/674
2. Drk, S., Puljko, A., Dželalija, M., & Udiković-Kolić, N. (2023). Characterization of Third Generation Cephalosporin- and Carbapenem-Resistant Aeromonas Isolates from Municipal and Hospital Wastewater. Antibiotics: volume 12, number 3, page 513
3. Shields R K, Chen L, Cheng S, Chavda KD, Press E G, Snyder A, and others (2017). Emergence of Ceftazidime-Avibactam Resistance Due to Plasmid-Borne blaKPC-3 Mutations during Treatment of Carbapenem-Resistant Klebsiella pneumoniae Infections. Antimicrobial agents and chemotherapy, volume 61, number 3
4. UKHSA (2023). Quarterly laboratory surveillance of acquired CPO in England: October 2020 to December 2022
Appendix
Appendix Table 1. QMLR returns for the total number of rectal swabs and faecal screening specimens taken for CPO screening by acute trust (England): January 2023 to December 2023
| Trust name | Trust type | Q1 2023 | Q2 2023 | Q3 2023 | Q4 2023 | |
|---|---|---|---|---|---|---|
| Airedale NHS Foundation Trust | Small | 2,161 | 327 | 381 | 359 | |
| Alder Hey Children’s NHS Foundation Trust | Specialist | 1,210 | 1,256 | 1,178 | 1,130 | |
| Ashford and St Peter’s Hospitals NHS Foundation Trust | Medium | 257 | 228 | 223 | 256 | |
| Barking, Havering and Redbridge University Hospitals NHS Trust | Teaching | 1,171 | 1,322 | 1,402 | N/r | |
| Barnsley Hospital NHS Foundation Trust | Small | 43 | 228 | 229 | 392 | |
| Barts Health NHS Trust | Teaching | 3,143 | 3,706 | 4,032 | 4,048 | |
| Bedfordshire Hospitals NHS Foundation Trust | Medium | 109 | 112 | 115 | 131 | |
| Birmingham Women’s and Children’s NHS Foundation Trust | Specialist | N/r | N/r | N/r | N/r | |
| Blackpool Teaching Hospitals NHS Foundation Trust | Teaching | 753 | 853 | 844 | 874 | |
| Bolton NHS Foundation Trust | Medium | 358 | 697 | 547 | N/r | |
| Bradford Teaching Hospitals NHS Foundation Trust | Teaching | 2,161 | 2,403 | 2,355 | 2,304 | |
| Buckinghamshire Healthcare NHS Trust | Multi-service | 315 | 473 | 549 | 606 | |
| Calderdale and Huddersfield NHS Foundation Trust | Large | 272 | 482 | 517 | 609 | |
| Cambridge University Hospitals NHS Foundation Trust | Teaching | 1,719 | 1,876 | 2,086 | 2,697 | |
| Chelsea and Westminster Hospital NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Chesterfield Royal Hospital NHS Foundation Trust | Small | N/r | N/r | N/r | N/r | |
| Countess of Chester Hospital NHS Foundation Trust | Small | N/r | N/r | N/r | N/r | |
| County Durham and Darlington NHS Foundation Trust | Multi-service | 161 | 917 | 1,905 | 3,410 | |
| Croydon Health Services NHS Trust | Medium | 493 | 119 | 199 | 210 | |
| Dartford and Gravesham NHS Trust | Small | 263 | 230 | 263 | 237 | |
| Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust | Teaching | 222 | 304 | 895 | 501 | |
| Dorset County Hospital NHS Foundation Trust | Small | 92 | 184 | 181 | 264 | |
| East and North Hertfordshire NHS Trust | Large | 1,144 | 1,252 | 1,439 | 1,437 | |
| East Cheshire NHS Trust | Small | N/r | N/r | N/r | N/r | |
| East Kent Hospitals University NHS Foundation Trust | Teaching | 328 | 462 | 526 | 499 | |
| East Lancashire Hospitals NHS Trust | Large | 351 | 509 | 452 | 491 | |
| East Suffolk and North Essex NHS Foundation Trust | Large | N/r | N/r | N/r | N/r | |
| East Sussex Healthcare NHS Trust | Large | 299 | 238 | 256 | 216 | |
| Epsom and St Helier University Hospitals NHS Trust | Teaching | 277 | 265 | 293 | N/r | |
| Frimley Health NHS Foundation Trust | Large | 679 | 793 | 2,221 | 2,707 | |
| Gateshead Health NHS Foundation Trust | Medium | 55 | N/r | N/r | N/r | |
| George Eliot Hospital NHS Trust | Small | N/r | 213 | 224 | 274 | |
| Gloucestershire Hospitals NHS Foundation Trust | Large | 129 | 131 | 214 | 204 | |
| Great Ormond Street Hospital For Children NHS Foundation Trust | Specialist | 1,747 | 1,715 | 1,692 | 1,641 | |
| Great Western Hospitals NHS Foundation Trust | Medium | 147 | 186 | 198 | 230 | |
| Guy’s and St Thomas’ NHS Foundation Trust | Teaching | 2,599 | 2,726 | 3,198 | N/r | |
| Hampshire Hospitals NHS Foundation Trust | Large | 380 | 258 | 779 | 657 | |
| Harrogate and District NHS Foundation Trust | Small | 109 | 101 | 100 | 143 | |
| Homerton Healthcare NHS Foundation Trust | Teaching | 854 | 892 | 939 | 1,158 | |
| Hull University Teaching Hospitals NHS Trust | Teaching | 211 | 219 | 1,002 | 789 | |
| Imperial College Healthcare NHS Trust | Teaching | 18,424 | 17,909 | 19,078 | N/r | |
| Isle of Wight NHS Trust | Multi-service | 35 | 44 | 53 | N/r | |
| James Paget University Hospitals NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Kettering General Hospital NHS Foundation Trust | Small | 238 | 316 | 287 | 218 | |
| King’s College Hospital NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Kingston Hospital NHS Foundation Trust | Medium | 100 | 257 | 216 | 335 | |
| Lancashire Teaching Hospitals NHS Foundation Trust | Teaching | 596 | 826 | 822 | 852 | |
| Leeds Teaching Hospitals NHS Trust | Teaching | 6,322 | 5,040 | 6,041 | 11,607 | |
| Lewisham and Greenwich NHS Trust | Large | 829 | 785 | 1,540 | 2,593 | |
| Liverpool Heart and Chest Hospital NHS Foundation Trust | Specialist | N/r | N/r | N/r | N/r | |
| Liverpool University Hospitals NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Liverpool Women’s NHS Foundation Trust | Specialist | N/r | N/r | N/r | N/r | |
| London North West University Healthcare NHS Trust | Teaching | 734 | 1,863 | 21 | 77 | |
| Maidstone and Tunbridge Wells NHS Trust | Large | 293 | 311 | 346 | 309 | |
| Manchester University NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Medway NHS Foundation Trust | Medium | N/r | N/r | N/r | N/r | |
| Mid and South Essex NHS Foundation Trust | Large | N/r | N/r | N/r | N/r | |
| Mid Cheshire Hospitals NHS Foundation Trust | Small | N/r | N/r | N/r | N/r | |
| Mid Yorkshire Hospitals NHS Trust | Large | N/r | N/r | N/r | N/r | |
| Milton Keynes University Hospital NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Moorfields Eye Hospital NHS Foundation Trust | Specialist | 0 | 0 | 0 | 0 | |
| Norfolk and Norwich University Hospitals NHS Foundation Trust | Teaching | 524 | 523 | 446 | 479 | |
| North Bristol NHS Trust | Large | N/r | N/r | N/r | N/r | |
| North Cumbria Integrated Care NHS Foundation Trust | Small | 1,030 | 1,163 | 600 | N/r | |
| North Middlesex University Hospital NHS Trust | Teaching | N/r | N/r | N/r | N/r | |
| North Tees and Hartlepool NHS Foundation Trust | Medium | 284 | 290 | N/r | N/r | |
| North West Anglia NHS Foundation Trust | Large | 151 | 207 | 216 | 104 | |
| Northampton General Hospital NHS Trust | Medium | 829 | 662 | 665 | N/r | |
| Northern Care Alliance NHS Foundation Trust | Teaching | 804 | 894 | 603 | 510 | |
| Northern Lincolnshire and Goole NHS Foundation Trust | Medium | 52 | 184 | 368 | 273 | |
| Northumbria Healthcare NHS Foundation Trust | Large | 185 | 225 | 235 | 264 | |
| Nottingham University Hospitals NHS Trust | Teaching | 1,732 | 1,696 | 2,136 | 2,215 | |
| Oxford University Hospitals NHS Foundation Trust | Teaching | 1,781 | 2,002 | 2,108 | 2,273 | |
| Portsmouth Hospitals University National Health Service Trust | Large | 246 | 264 | 268 | 323 | |
| Queen Victoria Hospital NHS Foundation Trust | Specialist | 0 | 6 | 0 | 3 | |
| Royal Berkshire NHS Foundation Trust | Large | 1,497 | 2,514 | 2,474 | 2,404 | |
| Royal Cornwall Hospitals NHS Trust | Large | 202 | 224 | 201 | N/r | |
| Royal Devon University Healthcare NHS Foundation Trust | Large | 192 | 330 | 448 | 390 | |
| Royal Free London NHS Foundation Trust | Teaching | 8,340 | 8,311 | 8,298 | 9,022 | |
| Royal National Orthopaedic Hospital NHS Trust | Specialist | 189 | 201 | 203 | 220 | |
| Royal Papworth Hospital NHS Foundation Trust | Specialist | 99 | 44 | 78 | 80 | |
| Royal Surrey County Hospital NHS Foundation Trust | Medium | 1,209 | 1,249 | 1,356 | 1,309 | |
| Royal United Hospitals Bath NHS Foundation Trust | Medium | 303 | 548 | 558 | 475 | |
| Salisbury NHS Foundation Trust | Small | 144 | 188 | N/r | N/r | |
| Sandwell and West Birmingham Hospitals NHS Trust | Large | N/r | N/r | N/r | N/r | |
| Sheffield Children’s NHS Foundation Trust | Specialist | 111 | 86 | 57 | 69 | |
| Sheffield Teaching Hospitals NHS Foundation Trust | Teaching | 1,127 | 1,138 | 1,499 | 1,487 | |
| Sherwood Forest Hospitals NHS Foundation Trust | Medium | N/r | N/r | N/r | N/r | |
| Somerset NHS Foundation Trust | Multi-service | 854 | 1,450 | 2,967 | 2,306 | |
| South Tees Hospitals NHS Foundation Trust | Teaching | 288 | 466 | 501 | 449 | |
| South Tyneside and Sunderland NHS Foundation Trust | Large | N/r | N/r | N/r | N/r | |
| South Warwickshire University NHS Foundation Trust | Medium | 533 | 638 | 903 | 931 | |
| Southport and Ormskirk Hospital NHS Trust | Small | N/r | N/r | N/r | N/r | |
| St George’s University Hospitals NHS Foundation Trust | Teaching | 988 | 1,176 | 1,096 | 1,206 | |
| St Helens and Knowsley Teaching Hospitals NHS Trust | Teaching | 1,274 | 1,634 | 1,612 | 9 | |
| Stockport NHS Foundation Trust | Medium | 388 | 427 | 397 | 371 | |
| Surrey and Sussex Healthcare NHS Trust | Medium | 252 | 265 | 233 | 285 | |
| Tameside and Glossop Integrated Care NHS Foundation Trust | Small | 192 | 253 | 234 | N/r | |
| The Christie NHS Foundation Trust | Specialist | 223 | 393 | 382 | 485 | |
| The Clatterbridge Cancer Centre NHS Foundation Trust | Specialist | N/r | N/r | N/r | N/r | |
| The Dudley Group NHS Foundation Trust | Medium | 40 | 39 | 30 | 54 | |
| The Hillingdon Hospitals NHS Foundation Trust | Small | N/r | N/r | N/r | N/r | |
| The Newcastle Upon Tyne Hospitals NHS Foundation Trust | Teaching | 670 | 1001 | 922 | 764 | |
| The Princess Alexandra Hospital NHS Trust | Small | 232 | 254 | 204 | 207 | |
| The Queen Elizabeth Hospital, King’s Lynn, NHS Foundation Trust | Small | 219 | 203 | 161 | 217 | |
| The Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust | Specialist | 104 | 126 | 42 | 46 | |
| The Rotherham NHS Foundation Trust | Small | 16 | 26 | 0 | 2 | |
| The Royal Marsden NHS Foundation Trust | Specialist | 128 | 202 | 112 | 209 | |
| The Royal Orthopaedic Hospital NHS Foundation Trust | Specialist | 385 | 412 | 329 | 342 | |
| The Royal Wolverhampton NHS Trust | Large | 2,219 | 2,525 | 2,777 | 2,970 | |
| The Shrewsbury and Telford Hospital NHS Trust | Medium | 114 | 104 | 152 | 112 | |
| The Walton Centre NHS Foundation Trust | Specialist | N/r | N/r | N/r | N/r | |
| Torbay and South Devon NHS Foundation Trust | Multi-service | 1 | 8 | 12 | N/r | |
| United Lincolnshire Hospitals NHS Trust | Large | 743 | 627 | 943 | 1193 | |
| University College London Hospitals NHS Foundation Trust | Teaching | 957 | 950 | 977 | 1064 | |
| University Hospital Southampton NHS Foundation Trust | Teaching | 647 | 1,290 | 771 | 804 | |
| University Hospitals Birmingham NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| University Hospitals Bristol and Weston NHS Foundation Trust | Teaching | 0 | N/r | 687 | 584 | |
| University Hospitals Coventry and Warwickshire NHS Trust | Teaching | 1,146 | N/r | 1,433 | 1,287 | |
| University Hospitals Dorset NHS Foundation Trust | Teaching | 170 | 224 | 178 | 232 | |
| University Hospitals of Derby and Burton NHS Foundation Trust | Teaching | 222 | 227 | 222 | 216 | |
| University Hospitals of Leicester NHS Trust | Teaching | 8,018 | 7,911 | 8,819 | 8,554 | |
| University Hospitals of Morecambe Bay NHS Foundation Trust | Teaching | 204 | 232 | N/r | N/r | |
| University Hospitals of Morecambe Bay NHS Foundation Trust | Teaching | 8,018 | 7,911 | 8,819 | 8,554 | |
| University Hospitals of North Midlands NHS Trust | Teaching | N/r | N/r | N/r | N/r | |
| University Hospitals Plymouth NHS Trust | Teaching | 919 | 888 | 997 | N/r | |
| University Hospitals Sussex NHS Foundation Trust | Teaching | 526 | 483 | 487 | 549 | |
| Walsall Healthcare NHS Trust | Small | 991 | 1,513 | 2,030 | 1,850 | |
| Warrington and Halton Teaching Hospitals NHS Foundation Trust | Teaching | 272 | 388 | 376 | 394 | |
| West Hertfordshire Teaching Hospitals NHS Trust | Medium | 836 | 0 | 957 | 1,046 | |
| West Suffolk NHS Foundation Trust | Small | N/r | N/r | N/r | N/r | |
| Whittington Health NHS Trust | Multi-service | 543 | 140 | 286 | N/r | |
| Wirral University Teaching Hospital NHS Foundation Trust | Teaching | N/r | N/r | N/r | N/r | |
| Worcestershire Acute Hospitals NHS Trust | Large | 2,074 | 2,199 | 3,031 | 3,054 | |
| Wrightington, Wigan and Leigh NHS Foundation Trust | Medium | 195 | 211 | 203 | 206 | |
| Wye Valley NHS Trust | Multi-service | 310 | 47 | 519 | 332 | |
| Yeovil District Hospital NHS Foundation Trust | Small | 1,083 | 1,173 | 2,248 | 1,258 | |
| York and Scarborough Teaching Hospitals NHS Foundation Trust | Teaching | 58 | 91 | 110 | 115 |
View this table in the data tables file
Acknowledgements
These reports would not be possible without the weekly contributions from microbiology colleagues in laboratories across England. The support from colleagues within UKHSA, and the AMRHAI Reference Unit in particular, is valued in the preparation of the report. Feedback and specific queries about this report are welcome via [email protected]