Group A streptococcal infections: fifth update on seasonal activity in England
Updated 29 June 2023
Applies to England

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/group-a-streptococcal-infections-activity-during-the-2022-to-2023-season/group-a-streptococcal-infections-fifth-update-on-seasonal-activity-in-england
Data to 1 January 2023.
Notifications and GP consultations of scarlet fever in England are currently showing exceptional levels of activity during this early point in the season further to public and healthcare professional alerts issued on 2 December 2022. Notifications of invasive group A streptococcus (iGAS) disease also remain higher than expected for this time of year.
Relatively high rates of iGAS in children continue to be noted. This may reflect increases in respiratory viruses and high levels of group A streptococcus (GAS) circulating in children.
Medical practitioners have been alerted to this early increase in incidence and elevated iGAS infection in children. Given the potential for severe presentations, scarlet fever cases should be treated promptly with antibiotics to limit further spread and reduce risk of potential complications in cases and their close contacts. Clinicians should continue to be alert to the severe complications of GAS and maintain a high degree of clinical suspicion when assessing patients, particularly those with preceding viral infection (including chickenpox) or close contacts of scarlet fever.
Interim clinical guidance on management of GAS infection has been issued to optimise diagnosis and treatment during this current increase in infection. Updated public health guidance on the management of close contacts of iGAS cases in community settings has been published, with additional groups now recommended for antibiotic prophylaxis.
As per national guidance, prompt notification of scarlet fever cases and outbreaks to local UK Health Security Agency (UKHSA) HPTs, obtaining throat swabs (prior to commencing antibiotics) when there is uncertainty about the diagnosis, and exclusion of cases from school or work until 24 hours of antibiotic treatment has been received, remain essential tools to limit spread.
Data presented within this seasonal activity update is based on that available as of 28 December 2022 and goes up to 1 January 2023 (the end of week 52). Delays in reporting are expected due to the bank holidays, therefore numbers presented in this report may change when updated data becomes available. A seasonal update report will be published later in January.
Weekly notifiable disease reports are published each week throughout the year to provide a regular update of scarlet fever notifications.
Key definitions are available at the end of the report.
Scarlet fever
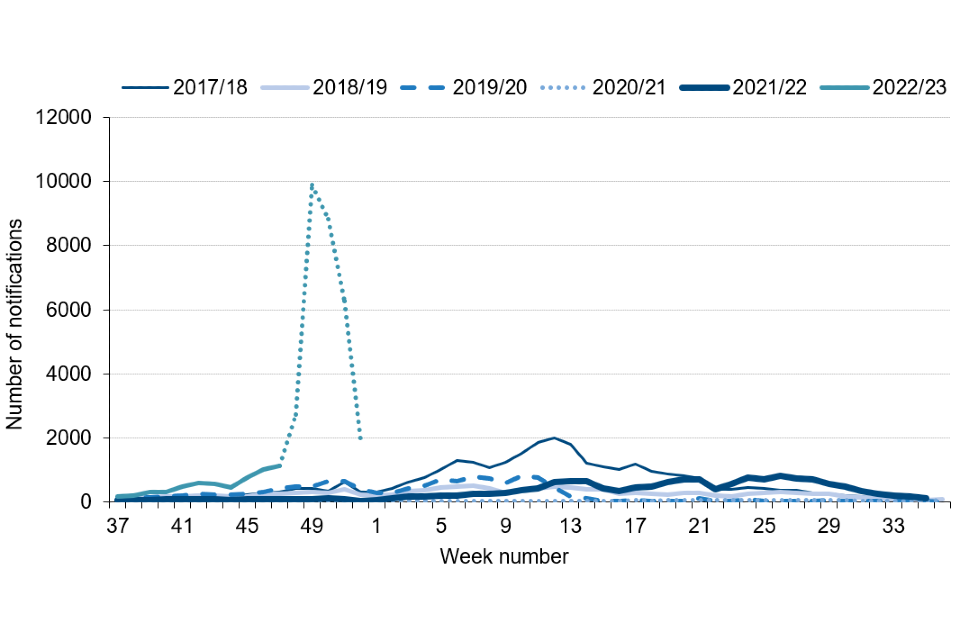
Following higher than expected scarlet fever activity during the early part of this summer in England, notifications during the early part of the current season (2022 to 2023; seasons are defined from week 37 (mid-September) to week 36 (mid-September)) increased to exceptional levels (Figure 1).
A total of 35,616 notifications of scarlet fever were received from week 37 to 52 of this season (2022 to 2023) in England, with a pre-Christmas peak of 9,899 notifications in week 49. This compares with an average of 2,861 (range 479 to 5,051) for this same period (weeks 37 to 52) in the previous 5 years (Figure 1). Increased health seeking behaviour as a result of national alerts is likely to have contributed to the increased reports. The last peak season for scarlet fever notifications was 2017 to 2018 when 30,768 reports were received across the entire season. A drop in notifications is noted for weeks 50 to 52, indicating a possible reduction in transmission rates, although potentially also reflecting delays in notification during the Christmas holidays.
Figure 1. Weekly scarlet fever notifications in England, by season, 2017 to 2018 onwards (weeks 37 to 52)
Note: In this graph the 2022 to 2023 season goes up to week 52 (1 January 2023). Recent weeks in the current season may change as further notifications are received, represented by a dotted line between weeks 47 and 52.
Scarlet fever notifications to date this season showed considerable variation across England, ranging between 46.4 (West Midlands) and 95.8 (East Midlands) per 100,000 population (table 1); while this may represent differential disease transmission it may also relate to differential notification practices by clinicians.
Table 1. Number and rate per 100,000 population of scarlet fever and iGAS notifications in England: week 37 to week 52 of the 2022 to 2023 season
Note: In this table, weeks 37 to 52 cover the period 12 September 2022 to 1 January 2023.
| Region | Number of cases of scarlet fever | Rate of scarlet fever | Number of cases of iGAS | Rate of iGAS |
|---|---|---|---|---|
| East of England | 3,466 | 51.8 | 127 | 1.9 |
| East Midlands | 4,659 | 95.8 | 117 | 2.4 |
| London | 4,814 | 53.5 | 159 | 1.8 |
| North East | 1,448 | 54.0 | 71 | 2.6 |
| North West | 5,951 | 80.8 | 160 | 2.2 |
| South East | 5,305 | 59.3 | 242 | 2.7 |
| South West | 3,208 | 58.3 | 171 | 3.1 |
| West Midlands | 2,766 | 46.4 | 110 | 1.8 |
| Yorkshire and the Humber | 3,999 | 72.4 | 176 | 3.2 |
| England | 35,616 | 63.0 | 1,333 | 2.4 |
Invasive group A streptococcal infection
Laboratory notifications of iGAS so far this season (weeks 37 to 52, 2022 to 2023) are higher than expected (Figure 2). A total of 1,333 notifications of iGAS disease received through laboratory surveillance in England, with a weekly high of 162 notifications in week 51 (19 to 25 December 2022). Laboratory notifications of iGAS infection are higher than recorded over the last 5 seasons for the same weeks (average 473, range 242 to 709 notifications; Figure 2).
Figure 2. Weekly laboratory notifications of iGAS, England, by season, 2017 to 2018 onwards (weeks 37 to 52)
Note: In this graph, the most recent weeks of the 2022 to 2023 season are expected to increase due to lags in reporting timelines from laboratories. The decline in recent weeks (week 52) should not be interpreted as an actual drop in laboratory notifications: Potential delays in reporting due to bank holidays is represented by a dotted line between week 50 and week 52.
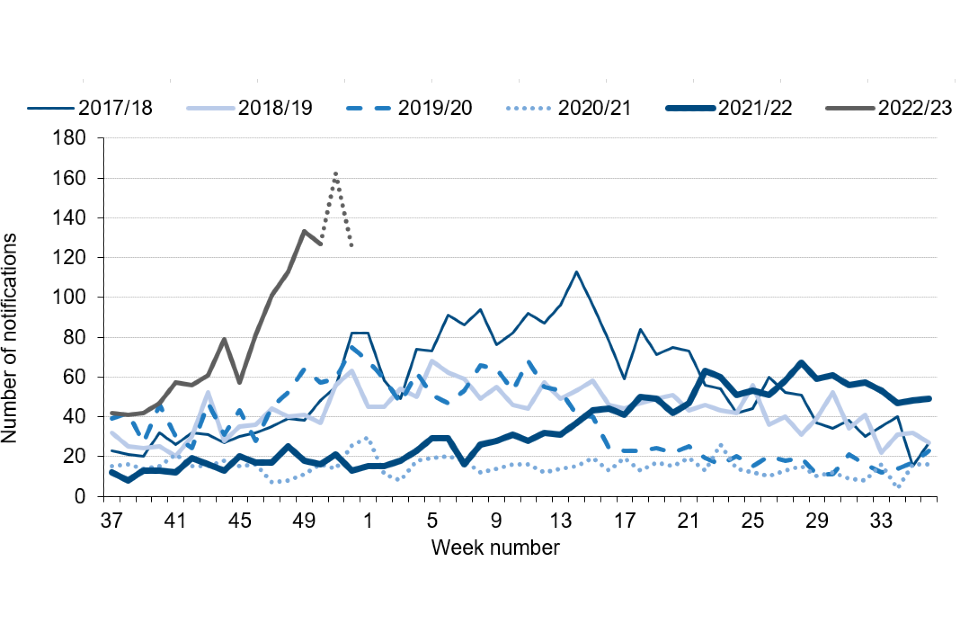
Weekly laboratory notifications are high for this point in the season and slightly higher than the weekly totals seen during the last peak season (2017 to 2018) when the peak weekly total was 113 in week 14 (2 April 2018 to 8 April 2018; Figure 2). A total of 1,207 notifications were received during a 14 week period during the last high activity year (weeks 5 to 18 in 2018), similar to the levels seen in the past 14 weeks (weeks 39 to 52; n=1,241). However, high levels of activity at such an early point in the season remain a concern, with further increases possible in the coming weeks.
During the current season to date, the highest rates were reported in the Yorkshire and Humber region (3.2 per 100,000 population), followed by the South West region (3.1 per 100,000) and the South West region (2.7 per 100,000); see Table 1.
The highest rate was in the 1 to 4 years age group (6.0 per 100,000), followed by those aged 75 years and over (5.7 per 100,000) and the under-1-year age group (2.7 per 100,000); see Table 2.
Table 2. Rate per 100,000 population of iGAS notifications in England by age group, weeks 37 to 52 in the 2022 to 2023 season versus the 2017 to 2018 season
Note: In this table the current 2022 to 2023 season covers weeks 37 to 52, whereas the 2017 to 2018 season data covers the full season, weeks 37 to 36.
| Age group (years) | 2022 to 2023 season (weeks 37 to 52): number of cases | 2022 to 2023 season (weeks 37 to 52): rate per 100,000 population | 2017 to 2018 (full season): number of cases | 2017 to 2018 (full season): rate per 100,000 population |
|---|---|---|---|---|
| Aged 1 year and under | 26 | 4.3 | 80 | 12.5 |
| 1 to 4 | 159 | 6.0 | 194 | 7.2 |
| 5 to 9 | 118 | 3.3 | 117 | 3.3 |
| 10 to 14 | 30 | 0.9 | 40 | 1.2 |
| 15 to 44 | 298 | 1.4 | 633 | 3.0 |
| 45 to 64 | 248 | 1.7 | 625 | 4.4 |
| 65 to 74 | 179 | 3.2 | 480 | 8.7 |
| 75 and over | 275 | 5.7 | 792 | 17.0 |
| Total | 1,333 | 2.4 | 2,967 | 5.3 |
The median age of patients with iGAS infection so far this season was 46 years (range 1 year and under, to 102 years), slightly lower than the range seen at this point in the preceding 5 seasons (age 53 to 57 years); 23% of iGAS infections reported so far this season are in children (aged 15 years and under), higher than the range seen for the past 5 seasons (4% to 13%).
So far this season 151 deaths have been recorded within 7 days of an iGAS infection diagnosis (from any cause), with 70% (n=107) of the recorded deaths being in those aged 45 years and over, and 15% (n=23) in children aged 10 years and under (Table 3). The case fatality rate (CFR) to date remains comparable this season to recent seasons. Elevations in rates of iGAS infection in children in this early part of this season have resulted in an increased number of deaths over a relatively short period, with 28 deaths in children aged under 15 in weeks 37 to 52. There have been 343 iGAS reports in children under 18 years in the season to date, with 29 deaths being recorded in this age group (CFR of 8.2%).
Antimicrobial susceptibility results from routine laboratory surveillance so far this season indicate tetracycline resistance in 13% of GAS sterile site isolates; this is lower than at this point last season (43%). Susceptibility testing of iGAS isolates against erythromycin indicated 4% were found resistant (compared with 20% last season) and, for clindamycin, 4% were resistant at this point in the season (15% last season). Isolates remained universally susceptible to penicillin.
Analysis of iGAS isolate typing data continues to indicate a diverse range of emm gene sequence types identified this season. The results indicate emm 1 was the most common (45% of referrals), followed by emm 12 (17%) and emm 89 (5%). In children (aged <15 years) emm 1 and emm 12 have dominated this season, accounting for 61% and 22% respectively.
Table 3. Case fatality rate (%) for deaths (all causes) within 7 days of an iGAS specimen, by age group in England for the current season and the previous 5 seasons
Notes: The total may include notifications where the age was unknown. The case fatality rate (CFR) is the percentage of deaths within 7 days of iGAS infection diagnosis for cases where follow-up has been possible. CFR should be interpreted with caution given the small numbers involved. The current season data (2022 to 2023) covers weeks 37 to 52 (12 September 2022 to 1 January 2023). The prior season’s data covers the whole season (weeks 37 to 36). ‘Pandemic seasons’ presents data for the 2019 to 2020 and 2020 to 2021 seasons combined.
| Age group (years) | 2017 to 2018 season % CFR | 2018 to 2019 season % CFR | Pandemic seasons (2019/2020 and 2020/2021) % CFR | 2021 to 2022 season % CFR | 2022 to 2023 season (weeks 37-52) % CFR | 2022 to 2023 season: number of deaths (all causes) within 7 days of iGAS |
|---|---|---|---|---|---|---|
| Aged 1 year and under | 5.6% | 2.1% | 7.7% | 3.8% | 4.3% | 1 |
| 1 to 4 | 4.7% | 6.1% | 9.0% | 5.9% | 7.9% | 12 |
| 5 to 9 | 9.9% | 4.6% | 2.7% | 10.6% | 8.8% | 10 |
| 10 to 14 | 7.9% | 8.7% | 23.8% | 0.0% | 17.9% | 5 |
| 15 to 44 | 4.1% | 1.7% | 2.5% | 2.3% | 5.6% | 16 |
| 45 to 64 | 8.4% | 8.6% | 9.3% | 9.7% | 8.9% | 21 |
| 65 to 74 | 13.5% | 8.8% | 13.8% | 13.1% | 16.6% | 28 |
| 75 and over | 24.4% | 16.8% | 19.9% | 18.1% | 21.4% | 58 |
| Total | 12.4% | 9.1% | 11.3% | 10.0% | 11.8% | 151 |
Discussion
While a recent downturn in scarlet fever notifications has been reported, rates of scarlet fever notification and GP consultations remain elevated. Weekly numbers of scarlet fever notifications this season have been higher than any previously recorded (weeks 49 to 52; weekly records available since 1982), the previous highest being in 2018. In the calendar year 2022, for England and Wales, there have been 54,419 scarlet fever notifications. The last year where there were higher notifications was in 1953, when there were 61,180 scarlet fever notifications in England and Wales.
The recent declines in scarlet fever notification since week 49 may represent reduced levels of transmission during the school holidays, often seen over the Christmas break, although delays in notification may also have played a role in reducing numbers. Very close monitoring will continue following the start of the school term to assess the impact on transmission.
The rate of iGAS infection notifications across the season showed a similar pattern of elevation, with weekly incidence trending above what would be expected during the first part of the season, particularly for recent weeks.
While the rate of iGAS infection is elevated in all age groups, incidence in children aged under 10 years is particularly elevated compared to levels reported in the last peak season, and substantially higher than in the past 2 years.
Investigations are underway following reports of an increase in lower respiratory tract GAS infections, particularly empyema, in children over the past few weeks. The current emm types have been circulating for many years. Whilst a new strain of emm1 (M1UK) was documented as having emerged and expanded in the last decade, its role (if any) in driving the current high levels of iGAS in children remains uncertain. At present, the weekly rate of iGAS in individuals over 75 years is not exceeding pre-pandemic periods and the CFR is lower than previous years, with emm1 dominant in this age group. Detailed genomic and biological investigations are underway to investigate any differences in the pathogen being seen this season.
The elevated iGAS levels in children compared to the period when pandemic control measures were in place is likely to be a consequence of the heightened scarlet fever activity given the crossover of strains associated in both presentations (1, 2). Reduced exposure to GAS infections during the pandemic are likely to have resulted in increased levels of susceptibility to these infections in children, noting the very low levels during pandemic. Prompt treatment of scarlet fever with antibiotics is recommended to reduce risk of possible complications and limit onward transmission.
Public health messaging to encourage contact with NHS 111 or GP practices for clinical assessment of patients with specific symptoms suggestive of scarlet fever has been issued along with reminders to provide ‘safety netting’ advice for parents indicating signs and symptoms of deterioration, particularly for children with respiratory viral infection. GPs and other frontline clinical staff are also reminded of the increased risk of invasive disease among household contacts of scarlet fever cases (3, 4).
Clinicians should continue to be mindful of potential increases in invasive disease and maintain a high index of suspicion in relevant patients as early recognition facilitates prompt initiation of specific and supportive therapy for patients with iGAS infection.
Relevant guidelines and information can be found on GOV.UK as follows:
- Guidelines for the public health management of scarlet fever outbreaks in schools, nurseries and other childcare settings
- Scarlet fever: symptoms, diagnosis and treatment
- Guidelines for the management of close community contacts of invasive GAS cases and the prevention and control of GAS transmission in acute healthcare and maternity settings
- Weekly notifiable diseases reports are published for a timelier update
- Group A strep – what you need to know (blog post)
Invasive disease isolates and also non-invasive isolates from suspected clusters or outbreaks should be submitted to:
Staphylococcus and Streptococcus Reference Section
Antimicrobial Resistance and Healthcare Associated Infections (AMRHAI)
UK Health Security Agency
61 Colindale Avenue
London
NW9 5HT
Data sources and methods
Scarlet fever notification data was extracted from the notifications of infectious diseases (NOIDs) reports, data for England was extracted on 4 January 2023. iGAS laboratory notification data was extracted from the UKHSA Second Generation Surveillance System (SGSS) and combined with specimen referrals to the Staphylococcus and Streptococcus Reference Section to produce a total number of episodes for England. Data was extracted on 3 January 2023.
The sharp increase in scarlet fever and other group A strep infections alongside increased awareness and vigilance amongst clinicians has led to a significant rise in scarlet fever notifications in recent weeks. This has resulted in a backlog of notifications of scarlet fever cases being entered into the national database after being processed.
A season runs from week 37 to week 36 each year (mid-September to mid-September). The 2022 to 2023 season data within this report covers 12 September 2022 to 1 January 2023.
All-cause deaths within +/- 7 days: reported date of death (obtained from tracing against the NHS SPINE where patient information is available) is compared to the date of iGAS specimen in a patient. This includes those where the difference between the 2 dates is ≤ 7 days, or ≥ minus 7 days (to include those potentially diagnosed via post mortem). Follow-up was not possible for all reported iGAS cases, primarily due to poor identifier (NHS number and date of birth) completion. In addition, not all iGAS cases have the full 7-day follow-up period for case fatality assessment. CFR should be interpreted with caution given the small numbers involved.
Population rates are calculated per 100,000 using the relevant year ONS mid-year population estimate.
The M protein gene (emm) encodes the cell surface M virulence protein.
Prior to the coronavirus (COVID-19) pandemic, there were a number of seasons with elevated incidence of scarlet fever and iGAS, in particular, the 2017 to 2018 season. This has been used as a comparison point to the trends in the current season. During the pandemic there was an unprecedented reduction in the number of scarlet fever and iGAS notifications, affecting the 2019 to 2020 season, and the 2021 to 2022 season.
References
1. Chalker V, Jironkin A, Coelho J, Al-Shahib A, Platt S, Kapatai G, and others (2017). ‘Genome analysis following a national increase in scarlet fever in England 2014’. BMC Genomics: volume 18 number 1, page 224
2. Al-Shahib A, Underwood A, Afshar B, Turner CE, Lamagni T, Sriskandan S, and others (2016). Emergence of a novel lineage containing a prophage in emm/M3 group A Streptococcus associated with upsurge in invasive disease in the UK’. mGen; volume 2 number 11
3. Lamagni T, and others (2018). ‘Resurgence of scarlet fever in England, 2014–16: a population based surveillance study’. The Lancet Infectious Diseases: volume 18, number 2, pages 180 to 187
4. Watts V, and others (2019). ‘Increased risk for Invasive Group A Streptococcus disease for household contacts of scarlet fever cases, England, 2011–2016’. Emerging Infectious Diseases: volume 25, number 3, pages 529 to 537
Acknowledgements
These reports would not be possible without the weekly contributions from microbiology colleagues in laboratories across England, without whom there would be no surveillance data.
The support from colleagues within UKHSA, and the AMRHAI Reference Unit in particular, is valued in the preparation of the report.
Feedback and specific queries about this report are welcome via [email protected]