Hand-arm vibration syndrome and assessment of vibration exposure
Updated 17 July 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/hand-arm-vibration-syndrome-and-assessment-of-vibration-exposure/hand-arm-vibration-syndrome-and-assessment-of-vibration-exposure
Presented to Parliament by the Secretary of State for Work and Pensions by Command of His Majesty
July 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit: nationalarchives.gov.uk/doc/open-government-licence/version/3.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at: www.gov.uk/official-documents.
Any enquiries regarding this publication should be sent to us at: [email protected]
ISBN 978-1-5286-4228-6
E02822108 07/23
Industrial Injuries Advisory Council
Dr Lesley Rushton, OBE, BA, MSc, PhD, Hon FFOM, (Chair)
Professor Raymond Agius, MD, DM, FRCP, FRCPE, FFOM
Professor Kim Burton, OBE, PhD, Hon FFOM
Professor John Cherrie, CFFOH
Ms Lesley Francois, LLB (Hons), MA, LLM
Dr Sally Hemming, CPsychol
Dr Max Henderson, MSc, PhD, MRCP, MRCPsych, Hon FFOM
DR Richard Heron, FRCP, FFOM
Dr Jennifer Hoyle, MRCP Edin, FRCP
Dr Ian Lawson, MB, BS, FFOM, FRCP, FRSPH
Professor Damien McElvenny, BSc MSc CStat CSci
Mr Steve Mitchell
Mr Daniel Shears, BA (Hons)
Dr Chris Stenton, BSc, MB, BCh, BAO, FRCP, FFOM, FFOM.RCPI
Dr Sharon Stevelink, BSc, MSc
Dr Gareth Walters, MD, FRCP, FHEA
Former Council Members
Mr Keith Corkan, BA
Ms Karen Mitchell, LLB
Mr Douglas Russell, BSc (Hons), MSc, CMIOSH
Dr A White, BSc (Hons), PhD, CMIOSH, AIEMA
HSE Observer
Ms L Darnton
IIAC Secretariat
Secretary: Mr S Whitney
Scientific Adviser: Mr I Chetland
Administrative Secretary: Ms C Hegarty
Dear Secretary of State,
Hand-arm vibration syndrome (HAVS) is a disorder resulting from prolonged exposure to vibration, specifically to the hands and forearms, while using vibrating tools. Symptoms include numbness, tingling, and loss of nerve sensitivity. HAVS is recognised as an occupational disease and is covered by prescribed disease PD A11 in industrial injuries disablement benefit.
The Industrial Injuries Advisory Council (IIAC) became aware, through correspondence and stakeholder engagement, that the PD A11 prescription may not reflect modern working-practices relating to occupation and vibrating tools used.
Consequently, IIAC embarked upon a review to establish how best to ensure the PD A11 was fit for purpose. On investigation, the Council found that there was a paucity of good quality epidemiological studies for extending the prescribed occupations for HAVS. The Council therefore decided to explore two alternative approaches.
The first involved a review of the assessment of vibration magnitudes, exposure response relationships and risk prediction modelling. A draft procedure for implementing this approach was developed, shared with external experts and departmental representatives and tested to see if it was practicable. Although this process demonstrated this approach could potentially be used to identify additional tools or processes, it became evident during the review, and from feedback received, that there were a number of practical drawbacks when applied to assessing individual exposure.
The second approach entailed consultation with external experts on the feasibility of an extension to the list based on their knowledge and experience of vibrating tools and the potential to develop hand-arm vibration syndrome. The Council felt that this approach was more suitable and following further consultation with external experts an extended list of vibrating tools was compiled to replace the existing list. As with current practice, the medical assessors will continue to determine whether vibration has been of sufficient intensity and duration when assessing PD A11 claims.
In its role of supporting the operation of the Scheme the Council will assist in the preparation of internal guidance on occupational history talking to assist medical assessors and will continue to review both epidemiological data and exposure data and where appropriate add further to this extended list.
A separate position paper accompanying this command paper, reviews the epidemiology on HAVS in more detail and outlines its limitations with regard to some occupational groups and vibrating tools.
Yours sincerely,
Dr Lesley Rushton
Chair, Industrial Injuries Advisory Council
Summary
Hand-Arm Vibration Syndrome (HAVS) can occur following exposure to Hand Transmitted Vibration (HTV) causing episodic finger blanching (the vascular component) and/or symptoms of numbness, tingling, reduced sensation and loss of dexterity of the fingers (the sensorineural component). The current prescription is defined in terms of HTV occurring following the use of a given list of tools and processes. The Industrial Injuries Advisory Council (IIAC) became aware that the current list diverged from other lists, including from the Health and Safety Executive (HSE).
The attribution of a disease to an occupation under the Industrial Injuries Disablement Scheme requires that there is evidence that work in the prescribed job or with the prescribed occupational exposures causes the disease with reasonable certainty i.e. on the balance of probabilities. In epidemiological terms this requires a more than doubling of relative risk.
On investigation, the Council found that there was a paucity of good quality epidemiological studies for extending the prescribed occupations for HAVS. The Council therefore decided to explore two alternative approaches.
The first involved a review of the assessment of vibration magnitudes, exposure response relationships and risk prediction modelling based on International Standard, ISO 5349-1. A draft procedure for implementing this approach was developed, shared with external experts and departmental (DWP) representatives and tested to see if it was practicable. Although this process demonstrated this approach could potentially be used to identify additional tools or processes, it became evident during the review and from feedback received that there were a number of practical drawbacks when applied to assessing individual exposure.
The second approach entailed consultation with external experts on the feasibility of an extension to the list based on their knowledge and experience of vibrating tools and the potential to develop hand-arm vibration syndrome. The Council felt that this approach was more suitable and following further consultation with external experts an extended list of vibrating tools was compiled to replace the existing list. As with current practice, the medical assessors will continue to determine whether vibration has been of sufficient intensity and duration when assessing PD A11 claims.
In its role of supporting the operation of the Scheme the Council will assist in the preparation of internal guidance on occupational history taking to assist medical assessors and will continue to review both epidemiological data and exposure data and where appropriate add further to this extended list. A position paper on epidemiological evidence for HAVS will be published separately.
Background
1. The council occasionally receives requests to review the terms of certain prescriptions in relation to the scheduled list of specified occupations or tasks and tools for a particular prescribed disease. This might follow an unsuccessful appeal or a referral by a stakeholder. Whilst avoiding comment on individual cases the Council has previously used relevant expertise on Council or sourced the available epidemiological evidence to decide if a more in-depth review might be required.
2. This has occurred on a number of occasions particularly with the physical agents list of prescribed diseases or section ‘A diseases’. Examples have included PD A10 (noise exposure from firearms and orchestral musicians), PD A11 (motorcycle handlebars), PD A14 (Osteoarthritis of the knee in tin miners).
3. More often than not, in these instances, epidemiological evidence is lacking or limited to case reports. Moreover, the likelihood of future relevant and sufficient epidemiological evidence being published is low. This limits the ability of the Council to establish attribution to the occupation of concern and, in particular, to determine its usual standard of evidence.
4. The purpose of this command paper is to explore whether alternative approaches to a reliance on the epidemiological evidence are feasible in relation to PD A11. One such approach would be the use of ‘equivalence’ i.e. to explore whether vibration exposures that have been shown in epidemiological studies to lead to a doubling of the risk of HAVS could be used as surrogate measures of risk for tools/activities for which there are no studies but where measures of vibration are available. An alternative approach would be to amend the current list of vibrating tools and equipment to include others, considered by expert opinion to be of equivalent risk to those on the current list.
The Industrial Injuries Disablement Benefit (IIDB) Scheme
5. The IIDB scheme provides a non-contributory, ‘no-fault’ benefits for disablement because of accidents or prescribed diseases which arise during the course of employed earners’ work. The benefit is paid in addition to other incapacity and disability benefits. It is tax-free and administered by the Department for Work and Pensions.
6. The legal requirements for prescription are set out in The Social Security Contributions and Benefits Act 1992 which states that the Secretary of State may prescribe a disease where they are satisfied the disease ought to be treated, having regard to its causes and incidence and any other relevant considerations, as a risk of the occupation and not as a risk common to all persons; and is such that, in the absence of special circumstances, the attribution of particular cases to the nature of the employment can be established or presumed with reasonable certainty.
7. Thus, a disease can only be prescribed if there is a recognised risk to workers in an occupation and the link between disease and occupation can be established or reasonably presumed in individual cases.
The Role of the Industrial Injuries Advisory Council (IIAC) and prescription
8. IIAC is an independent statutory body established in 1946 to advise the Secretary of State for Social Security on matters relating to the IIDB scheme.
9. Much of the Council’s time is spent considering whether the list of prescribed diseases for which benefit may be paid should be enlarged or amended. The Council searches for a practical way to demonstrate, in the individual case, that the disease can be attributed to occupational exposure with reasonable confidence. For this purpose, ‘reasonable confidence’ is interpreted as being based on the balance of probabilities.
10. Some occupational diseases are relatively simple to verify, as the link with occupation is clear-cut. Some diseases only occur due to particular work, or are almost always associated with work, or have specific medical tests which prove their link with work, or have a rapid link to exposure, or other clinical features that make it easy to confirm the work connection. However, many other diseases are not uniquely occupational, and when caused by occupation, are indistinguishable from the same disease occurring in someone who has not been exposed to a hazard at work. In these circumstances, attribution to occupation depends on research evidence that work in the prescribed job or with the prescribed occupational exposures causes the disease on the balance of probabilities. The Council thus looks for evidence that the risk of developing the disease associated with a particular occupational exposure or circumstance is more than doubled. (Previous reports of the Council explain why this threshold was chosen.)
11. This command paper will explore some proposed alternatives i.e. identifying indirect rather than direct evidence of a doubled risk. It should be stressed that this would only apply where there is already established epidemiological evidence of a doubling of risk for some tools or occupations but lacking for others (where the Council has reviewed the extant epidemiological evidence). Included in this review is an exposure response model, used to assess equivalent exposure to those tools and processes already on the list of scheduled occupations. The model has the potential for use as an approximation of exposure or as a complement to expert opinion, epidemiological evidence and clinical assessment.
Hand-arm Vibration Syndrome
12. A number of disorders affecting the upper limbs are associated with hand-transmitted vibration (HTV), the main one being ‘Hand-arm Vibration Syndrome’ (HAVS). This includes a form of Raynaud’s phenomenon called vibration-induced white finger (VWF) and digital neuropathy, an injury to nerves supplying the fingers and thumbs. Carpal tunnel syndrome (CTS) (an entrapment of a nerve supplying sensation to the hand) is another well-recognised complication of HTV exposure (PD A12) (Command paper, Cm 6868). Long term exposure to HTV under defined conditions can also lead to Dupuytren’s contracture (PD A15) (Command paper, Cm 8860). Affected individuals may have one or several of these disorders. Affected individuals may have one or several of these disorders. Long term exposure to HTV under defined conditions can also lead to Dupuytren’s contracture (PD A15) (Command paper, Cm 8860).
Raynaud’s phenomenon
13. Raynaud’s phenomenon is characterised by episodes of finger-blanching due to temporary interruption of blood flow to the extremities of the digits. During an episode, the extremity becomes cold, numb and marble white or blue. Typically, attacks are triggered by the cold. During the recovery phase, as the circulation restores, the affected parts become fiery red and tingle.
14. Primary Raynaud’s phenomenon arises naturally in some 5-10% of men and 10-20% of women, with some variation in disease frequency by race, climate, geography and case definition. Less commonly, Raynaud’s phenomenon can be secondary to certain rheumatic diseases, blood disorders and drugs, or can arise from traumatic injury. With stricter criteria lifetime prevalence approximates to 5% (Palmer, 2000, Garner 2015).
History of Prescription of PD A11
15. Prior to considering any alternative approaches, an understanding of the provenance of the current list of tools and processes in PD A11 should be covered. The current prescription for A11 includes a list of tools and their occupational use (Appendix 1). The first reference to a list of tools occurs over 40 years ago in the Command paper on VWF published in 1981 (Cm 8350). This list was compiled from evidence received from experts and the Health and Safety Executive (HSE) which appeared to ‘expose workers to the greatest risk’ and led to the recommendation by IIAC to add VWF to the list of prescribed diseases. Although the wording of the list has altered slightly it remains largely based on the original evidence (Appendix 1.
16. Comparing the list of scheduled occupations with the current list produced by the HSE of jobs and tools likely to involve hand-arm vibration, highlighted a divergence in some areas e.g., the HSE list includes hedge trimmers and powered mowers (Appendix 2.
17. The Council reviewed the evidence again in 1995 (Cm 2844) and recommended not only the inclusion of the sensory component (renaming VWF as hand-arm vibration syndrome, HAVS), but a more extensive list of tools and processes (Appendix 3). The Council ‘…agreed that prescription based on vibration measurement of a list of specific tools was not practical and that extension of the scheme to groups of tools needed to be considered. The list of prescribed occupational exposures should be replaced by tools listed in Appendix 4 and rigid materials held against such tools’. These recommendations were not enacted, and the original list has remained in place.
18. The most recent review of occupational exposure was undertaken in 2004 (Command paper Cm 6098 paragraphs 61-67): ‘Ideally, coverage would be broader, relating to the extent of exposure to hand transmitted vibration (HTV), estimated as a dose. This appears to be too difficult in practice’. The report makes reference to the recommended list in the 1995 Command paper but also emphasises the point that the risk of HAVS amongst several other variables (i.e. grip force and hardness of workpiece materials) depends on both the magnitude of hand transmitted vibration and the duration of use of these tools: ‘Research indicating that such exposures directly translate into a doubling of risk of HAVS in human populations was rather sparse’. The conclusion was that there was insufficient weight of epidemiological evidence to modify the terms of occupational coverage (apart from amendment to the use of hand-held chains saws in forestry).
19. Of note is that the current list does not include an exposure duration. If the occupational criteria are satisfied, the Decision Maker (DM) will refer the claimant for a full medical assessment where the exposure history and duration of exposure will be assessed in more detail. However, if the occupational criteria are disallowed a medical assessment will not take place. The only exception is when an activity is performed only occasionally or in an incidental way.
20. To make a diagnosis of HAVS requires three criteria to be satisfied (Montracon v Whaley 2005):
a. a history of exposure to vibration sufficient to cause a risk of development of the condition (HAVS)
b. a clinical history and description of symptoms which is consistent with one or more components of HAVS
c. the absence of any constitutional explanation for the symptoms.
Criteria b) and c) were reviewed in IIAC Position Paper 43 (2019). What constitutes ‘sufficient’ in this context includes both the intensity and duration of vibration exposure.
The assessment of vibration intensity, duration and associated limitations
21. Intensity of vibration for different tools is usually measured as an acceleration unit corrected for an eight hour working day and referred to as an ‘A(8)’ value. More detail on hand transmitted vibration and how this is measured and calculated is given in Appendix 4. There are a number of international standards with defined criteria for obtaining an accurate measurement of vibration. However, it is acknowledged that, for various tools, measurement can lead to a range of values which are affected by a number of factors including ergonomic aspects of the work, hardness of workpieces and tool maintenance. The key standards in the measurement of vibration are ISO 5349 parts 1 and 2 (ISO 5349, 2001, see Appendix 4.
22. The duration of vibration exposure is usually recorded in years or cumulative hours. In practice several different tools are often used by a worker for variable periods of time per day and per year, so any assessment is influenced by the accuracy of worker recall.
23. Another issue is the intermittency of exposure and gaps or significant periods of say years without any exposure. In this situation an estimate of ‘dose equivalence’ can been made:
dose = Σ[footnote 1] A(8)t
where t is either an estimate of the total years of exposure or the sum of hours/day + days/week + weeks/year).
Alternative forms of assessing dose have been proposed (VIBRISKS, 2007).
24. The assessment of whether an individual has developed symptoms attributable to HAVS relies on combining an appropriate personal clinical history with a detailed occupational history of vibration exposure. The Council has previously recognised that there can be individual variations in the pattern of clinical development in HAVS (Position Paper 43, 2019). Likewise, the determination of sufficient vibration exposure in an individual worker should not be limited to a defined ‘cut-off’ level of vibration magnitude or duration of exposure. Any consideration of an alternative approach involving a dose response relationship needs to acknowledge the potential for variation in individual responses and workplace tasks.
Exposure response relationships and risk prediction modelling (ISO 5349-1)
25. Assessing the exposure response relationship between the use of vibrating tools and HAVS is not straightforward. Whilst increasing intensity and duration of exposure may lead to the onset and increasing severity of HAVS, the relationship is not a linear one. Both the intensity (vibration magnitude A(8) and duration of exposure (cumulative years) are important.
26. As outlined above assessing vibration dose requires knowledge of three variables: the vibration magnitude, the daily usage and the years of exposure to vibrating tools. The response aspect is complicated by the syndromic nature of HAVS having both neurological (peripheral neuropathy) and vascular (VWF) components developing separately albeit usually concurrently. Vascular only HAVS and sensorineural only HAVS, although less frequent, do occur. An exposure response relationship derived from the analysis of epidemiological studies of vibrating tools in the vibration frequency range 30 Hz to 50 Hz (e.g., chain saws, grinders, rock drills) is included in ISO 53491 Annex C. The model includes the three variables and estimates a dose-response relationship with the onset of white finger or finger blanching as the response measure. There is an inverse relationship between the exposure time (in years, Y) for the onset of finger blanching (also referred to as the ‘latent interval’) and vibration magnitude A(8) (Appendix 4 shows a more detailed equation). Griffen (2008) pointed out that the relationship between these parameters suggests a degree of precision that does not take account of those leaving and entering the group and suggested a more reasonable estimate for duration of exposure (in a range 1-25 years) is given by the equation:
Y10% ≈ 30/A(8)
Y is the number of years that produces 10% finger blanching in a group for a particular vibration magnitude A(8).
See Appendix 4 for further details on this equation.
27. As noted earlier, it is generally accepted that constitutional Raynaud’s occurs in 5% of men and 15% of women. Assuming a 5% level, then a group with a 10% prevalence would be double the expected rate. For example, an A(8) value of 3.7 ms-2 would give a 10% prevalence after 8 years, while an A(8) of 14 ms-2 would give a 10% prevalence in just 2 years. The HSE Exposure Action Value (EAV) of 2.5 ms-2 would give a 10% prevalence in 12 years. It is important to state that there is no dose-response model for the sensory aspects of HAVS so ‘sensory only’ HAVS would be a problem with this model.
Uncertainties in the use of the exposure response model
Variability in individual susceptibility
28. As stated above ISO 5349-1 accepts that the probability of individuals developing symptoms also depends on their susceptibility and any personal factors, pre-existing diseases and ergonomic factors. In this context the model is assumed to apply to a group that are similarly exposed and was not intended for use in individual assessments. ISO 5349-1 (Annex C) also noted that symptoms of HAVS are rare in persons exposed to an 8-h energy-equivalent vibration total value, A(8), at the surface in contact with the hand of less than 2 ms-2 and unreported in A(8) magnitudes of less than 1ms-2 (see Appendix 4). Although 1ms-2 may be referred to as a ‘de minimus’ or safe level in civil cases it is not accepted by all authorities and HAVS has been reported at exposures between 2 ms-2 and 2.5 ms-2 (Burström 2006). Griffin, when reviewing HTV standards in a Handbook of Human Vibration, stated that ‘..simple vibration limits can be unreasonable because it is impossible to define a numerical value beyond which there is certainty of injury and below which there is no possibility of injury’ (Griffin 1990).
29. There is a large variation in individual susceptibility to HTV where one worker may develop symptoms after a year while others may take 30 years despite being similarly exposed (Griffin 2008).
30. A critical review of the evidence related to hand-arm vibration syndrome and exposure to vibration was undertaken by the Health and Safety Laboratory (HSL) (HSL RR1060 2015). The report included a discussion on the strength of evidence found relating to frequency weighting, biological effects and health outcomes. The HSL made a number of evidence statements and questioned the universal use of ISO 5349-1. It was noted that ISO 5349-1 assumes the daily exposure is the same throughout the working lifetime. The conclusion stated that ‘This review has found no strong evidence that establishes precise quantitative relationships between exposure to vibration and associated health outcomes, including the key well-recognised endpoints of vascular or neurosensory HAVS.’
Suitability of the weighting system used in ISO 5349-1
31. ISO 5349-1 employs a frequency weighting (Wh) system based on small-scale experimental studies of sensitivity thresholds and equal sensation contours (Miwa, 1967) without epidemiological, pathological or physiological evidence. This potentially overestimates the risk from tools that vibrate at lower frequencies (<16Hz e.g. percussive tools such as road breakers) and underestimates risk in intermediate at higher frequencies (16-250 Hz e.g. rotary tools such as grinders or drills).
32. A physiological study of the acute vascular responses to vibration suggested increasing sensitivity in the frequency range 16-250 Hz (Bovenzi, 2000). Biodynamic studies found that the response of the hand-arm system is frequency-dependent in that it is different in the fingers and hand compared to wrists and elbows (Dong, 2004, 2005). Another epidemiological study also suggested possible improvements to both frequency weighting and time dependency used to predict the onset of VWF (Griffin 2003). Krajnak concluded that the risk of injury to the fingers and hands was greatest at a frequency >100 Hz (Krajnak et al 2012).
33. In addition, ISO 5349-1 states that ‘It is not known whether this frequency weighting [Wh] represents, separately, the hazard of developing vascular, neurological or musculoskeletal disorders. At present, it is used for the assessment of all biological effects of hand transmitted vibration.’
34. In later epidemiological studies Bovenzi (Bovenzi, 2011, 2012, 2019) compared alternative frequency weighting systems with ISO-5349-1. In the latest 2019 study, an alternative weighting was found to be more appropriate for the intermediate and higher frequencies. The alternative frequency weighting (Wp) used in the study was based on the biodynamic, pathophysiological and epidemiological evidence proposed in ISO Technical Report, ISO/TR 18570-2017 (Appendix 4). However, ISO/TR 18570 was only ever intended for use in data collecting and research purposes. In addition, commercially available vibration measuring devices do not contain filters that account for Wp weighting in the magnitude measurements. Vibration magnitudes for this alternative weighting of tools would need to be sourced to make this model of any practical value.
Approach 1: Application of the ISO 5349-1 model as an approach to assessing exposure equivalence for HAVS
35. As indicated the ISO 5349-1 model was compiled from epidemiological data (chain saws, grinders, and rock drill workers) and therefore was assumed to apply to a group of workers and not intended for use on an individual basis. However expert opinion is that despite the caveats highlighted above higher exposure assessed according to ISO 5349-1 generally indicate a higher risk of developing HAVS. The Control of vibration at Work Regulations (CVAWR, 2005) defines daily vibration in terms of ISO 5349-1 and similarly the HSE makes enforcement decisions based on this method. With the caveats described above in mind the Council explored the potential for an alternative approach using the ISO 5349-1 model above to assess an approximate equivalence 11 level of vibration dose of other tools for example strimmers to those tools and processes already on the scheduled list.
36. It should be noted the Council considered exposure equivalence previously as a suitable approach for the extension of the terms of prescription for Occupational Deafness (Position Paper 38 (2017)) 37. However, Command Paper 6098 (paragraph 18 above) referred to the difficulty in assessing tool use and individual exposures to HTV. Vibration magnitudes A(8) in isolation may not assist in determining an equivalent to a doubling of relative risk. It was also noted the Council rejected the use of vibration magnitudes more recently in 2017 when assessing HAVS occurring from vibrations of motorcycle handlebars (Information note 2017). Essentially, the view was that there were too many uncertainties around the dose-response assessment and a wide variation in vibration levels recorded for the same type of tool.
38. The use of the exposure response equation requires the ready availability of data on vibration magnitudes of commonly used tools. A potential claimant would be required to provide details of the tools used and information on the frequency and duration of use of these tools.
39. There are numerous detailed guides on vibration exposure assessment. The most common exposures that a worker will experience come from a variety of tools and processes that vary both daily and throughout a working life. Calculators of A(8) values have been developed to assist with assessing daily individual exposures.
40. Alternatively, rather than seeking to find a threshold level of risk or trying to assess individual exposures at the occupational exposure stage, the Council explored whether it was possible to compare vibration magnitudes of a similar order of magnitude from any new requests with those on the current list.
41. Information about tool vibration magnitudes and their ranges have been reported since the 1995 and 2005 command papers, allowing a comparison of the Scheme list with median levels of vibration for a variety of tools. The current list of types of jobs and tools have been accepted for the doubling of risk from epidemiological data, but they will also have all the uncertainties described above about using HTV (such as range of measurements for individual tools, workpiece hardness, or effect of maintenance programmes) that are effectively used to reject the use of vibration magnitudes in any new requests. A list of tool vibration ranges has been complied by the HSE.
42. One way of adding to the list of jobs or processes eligible for PD A11 is to accept those with documented equivalent A(8) vibration magnitudes that could lead to 10% prevalence in line with ISO 5349-1. If an employer’s risk assessment under the Control of Vibration at Work Regulations 2005 shows that if there is exposure above the HSE’s EAV, then that could be taken as evidence of an A(8) of 2.5 ms-2 or more. The occupational history during the subsequent medical assessment could then refine the exposure details and estimate whether the cumulative exposure has been sufficient to lead to the onset of vascular HAVS.
43. The Council therefore explored the possibility of a standalone procedure based on ISO 5349-1 for use by Decision Makers to assess vibration exposure for tools or processes not currently on the list of scheduled occupations i.e., effectively determining whether there is an equivalent level of exposure to those tools and processes already prescribed. A 3-step protocol was devised where the claimant would firstly list tools used and daily exposures which are then compared with an HSE list of tools of known vibration magnitudes. An HSE Hand-Arm Vibration Exposure Calculator (para 39) can then be used to calculate the total A(8) value and then finally an equation is used to determine if the reported years of exposure (Y) are sufficient to create a doubling of percentage risk (10%), where Y10% ≈ 30/A(8). A list of Y10% for various A(8) values and worked examples were compiled. The model would potentially lead to a greater number of occupations referred for a medical assessment.
44. It was recognised that this proposed exposure equivalence model essentially introduces three new independent variables of vibration dose (magnitude, daily usage and years of exposure) that are not a feature of the current list of scheduled occupations. However, the original intention was not to alter the approach with the current list but allow a surrogate measure for tools not currently prescribed to progress to a medical assessment. The purpose of introducing these variables is to ask whether the onset of blanching is ‘more likely than not’ caused by vibration and consistent with the reported exposure.
45. The onus would be on the claimant to provide details of tools used along with years of exposure. This would be very different to the limited detail required by the current list. Vibration magnitudes from suppliers’ data would have to be obtained if the tools are not currently included in the HSE calculator or list. The employers’ duty to carry out risk assessments as part of the CVAWR 2005 regulations may be a resource for vibration magnitudes, although these assessments may not have sufficient detail on magnitudes. Suppliers’ data on vibration magnitudes is another potential resource, but these only provide vibration emission data as opposed the more pertinent ‘in-operation’ A(8) values. An additional problem is that of recall and a potential for bias in terms of either tools used or years of exposure.
46. Employee and employer assessment of daily exposure hours often varies significantly with employees generally overestimating ‘trigger time’ (time spent actually working with the tool) and employers tending to underestimate it. A study by Palmer (Palmer, 2000) of self-reported occupational exposure to HTV found that employees overestimated their duration of exposure by a factor of 2.5 (interquartile range 1.6-5.9). A study of dental hygienists using a daily diary and interview found that they overestimated their exposure on average by between 3 and 8 times respectively (Akesson, 2001). Another study of grinders concluded that estimates of grind wheel consumption had a better correlation with exposure by ISO 5349-1 than by workers reports which was almost four-fold higher (Gerhardsson, 2005). Clear guidance on the concept of ‘trigger’ time may help to overcome some of these issues of ascertainment bias.
47. There are currently no limits on the length of time that a claimant must have been employed in any of the scheduled occupations, although Decision Makers should be satisfied that the time using relevant tools or materials is a regular part of their job. The HSE produces operational guidance of internal instructions used by inspectors to carry out its core operational work (HSE,2020). This defines regular and frequent use as “repeated several days each week over months and years”. The guidance also provides some advice for employers when carrying out risk assessment to determine whether the Exposure Action Value (EAV) is likely to be exceeded: 1 hour per day for rotary tools (e.g. grinders, polishers, chainsaws) and 15 minutes for percussive tools (e.g. breakers, scabblers, chipping hammers). This is based on time to reach the EAV for assumed tool vibration magnitudes of 7 ms-2 and 10 ms-2 respectively. However, the application of this approach in the context of the scheme, with the potential variety for tools involved is also likely to be impractical. Tools with similar vibration magnitudes can lead to a wide range in latency periods before the onset of symptoms.
48. The draft procedure was shared with external experts, staff from the Department of Work and Pensions and medical assessors to test whether it was practicable. External experts indicated that whilst the model may have some merits it would be too onerous for Decision Makers to apply in practice. This was echoed by feedback from Decision Makers, Operations, and medical assessors. The main concerns identified in summary were:
- under-or over-estimation of risk
- problems in accounting for individual susceptibility
- burden of additional information gathering
- problems ascertaining reliable information on tools
- problems with recall of exposure leading to bias
49. Whilst this exercise was useful and informative because of the practical considerations outlined in paragraph 48 the Council decided to rule this approach out. In addition to avariation in individual sensitivity there are other challenges in making a diagnosis of HAVS that would preclude using a fixed cut-off of vibration magnitude or years of exposure to assess sufficiency of exposure. How this aspect can be problematic and its relation to an assessment in PD A11 is explored further in Appendix 5.
Approach 2: Extension of the list of tools using expert opinion
50. Previously the Council has looked at individual requests to add to the list of tools or occupations e.g., motorcycle handlebars (Information note 2017). Rather than looking at specific examples the Council decided to re-visit the possibility of extension of the list of occupations e.g., the HSE list (Appendix 2), the proposed list in the 1995 Command paper (Command paper Cm 2844, Appendix 3) or simply use term ‘hand14 held vibrating tools’? It would then be up to the medical assessors to assess whether there has been vibration exposure of sufficient severity and duration.
51. Two external experts were asked for their opinion, firstly on whether the list should be extended and secondly whether the list of occupations should be added to where there is some epidemiological evidence of an increased risk but not sufficient to confirm ‘a more likely than not’ question and supplemented with knowledge of vibration magnitudes equivalent to exposures of those tools currently on the list.
52. They were in favour of extending the list but not limiting it to the term ‘hand-held’ vibrating tools or to a list of occupations or processes. The current list in PD A11 is a combination of occupations or processes. The Health and Safety Executive guidance recognises that there can be significant risk from exposure to HTV from hand-held, hand-guided and hand-fed machines. The list in Command paper Cm 2844 contains examples of all three (Appendix 3). Also, the current HSE table of common vibrating tools (listed in appendix 3 to the second edition of L140, 2019) was considered to be a good starting point for an extension to the list for PD A11.
53. In addition, the experts also advised against limiting the terms of prescription, as in the current list, to how tools or machines are used i.e., qualifying that a grinder must have been operated on metal.
54. The experts felt that there should be no discrimination against an occupation that is shown to involve significant vibration exposures but which for lack of data has no epidemiological evidence of increased risk. Exposure evidence is used by HSE as a surrogate for evidence of disease.
55. Therefore, the Council explored this approach further, working with external experts to prepare a new list which would contain examples of all three types of tools. The experts also recommended a definition of what is regarded as “regular and frequent” use. They cited the example used by HSE that defines regular and frequent use as “repeated several days each week over months and years”. (See paragraph 47.
56. However, this was considered too problematic for Decision Makers to apply in practice without a clear cut-off in terms of years of exposure. In addition, it is not appropriate or practicable to establish a list of typical or average vibration magnitudes for all the categories of tools. It would be more preferable to prepare a list with broad ranges of vibration magnitudes. The intention is not to use these as fixed ‘threshold level’ values to decide sufficiency of exposure but as guidance to demonstrate the broad range of potential magnitudes for unfamiliar tools to assist the medical assessments (Appendix 5).
57. Where a condition is clinically indistinguishable from the same disease caused by factors outside work, attribution to work in a claimant with both occupational and nonoccupational risk factors rests on a detailed assessment of causal probabilities and on the research evidence base, rather than on clinical judgement. In this respect Prescribed disease PD A11 currently benefits from presumption. Causation of PD A12, carpal tunnel syndrome and more recently PD A15, Dupuytren’s contracture, the generic term hand-held vibrating tools has been adopted. However, the lack of a dose response relationship in the former means that PD A12 does not have the benefit of presumption. A15 has this benefit but has a more clearly defined exposure duration. The combined generic term ‘hand-held vibrating tool’ recognises that separating out vibration hazards from ergonomic hazards is rarely addressed in epidemiological studies (Lawson, 2020). The rule of presumption will continue for tools that were on the extant list but excluded from those tools added to the new list.
Conclusions
58. The Council recognises that epidemiological studies in occupations that could lead to additions to the list of scheduled occupations in a number of prescribed diseases is often deficient.
59. This command paper specifically looked at vibration magnitudes of tools and processes and the potential assessment of equivalence to the list of scheduled occupations in PD A11.
60. One approach was to propose a model for assessing equivalent exposure that was comparable to a doubling of risk. A second approach involved a consultation exercise with experts on the feasibility of extending the list of vibrating tools and equipment that have the potential for hand-arm vibration syndrome to develop.
61. As part of the first approach a simple three step procedure (based on ISO 5349-1) for use by Decision Makers was developed to approximate whether the occupation question on vibration exposure could be satisfactorily assessed for tools not on the current scheduled list of occupations. This would allow progression for a medical assessment on tools not in the current list.
62. It was evident from this review that a model based on ISO 5349-1 derived from the analysis of groups of workers to assess individual exposure had a number of drawbacks. Feedback from external expertise and internal stakeholders indicated that the model was not practicable.
63. It was concluded that an exposure equivalence approach, by use of the model, in this instance was not robust enough for the calculation of a meaningful estimation of dose at the occupation question stage and may be ‘unsafe’ and problematic to implement in practice. However, the concept of investigating exposure equivalence may be adopted in other prescribed diseases where the epidemiological evidence is limited.
64. The second approach entailed consultation with external experts with questions on the feasibility of extending the list based on their knowledge and experience of vibrating tools with the potential to lead to hand-arm vibration syndrome. Information on a wider range of tool vibration magnitudes is more readily available than when an extended list of tools and processes was recommended in Cm 2844, 1995.
65. An extended list of vibrating tools and equipment was compiled with external expertise with the intention of replacing the existing list in Schedule 1. The list of tools is separated by categories with examples of specific tools in each. Guidance will be prepared with a longer list of tools in each category. Those tools used in occupations or processes in the current terms of prescription would continue to benefit from presumption having been determined by epidemiological research. Any of the tools in the new recommended list not supported by epidemiological or insufficient epidemiological evidence (that were not included in the previous list) would not benefit from the presumption rule. The Council will keep the research evidence under review and amend the presumption rule as necessary should evidence of a doubling of risk emerge on new tools. As with current practice the medical assessors will continue to determine whether vibration has been of sufficient intensity and duration when assessing PD A11 claims. This would make it easier for both claimants and assessors.
Recommendations
66. The recommendation of the Council is to replace the current scheduled list with a list of tools and processes. With support from external experts an expanded list has been developed with recommendations to amend the wording in Schedule 1 in PDA11 to as follows:
| Recommendation | Health condition | Tools and processes |
|---|---|---|
| A11 | a) Intense blanching of the skin, with a sharp demarcation line between affected and non-affected skin, where the blanching is cold-induced, episodic, occurs throughout the year and affects the skin of the distal with the middle and proximal phalanges, or distal with the middle phalanx (or in the case of a thumb the distal with the proximal phalanx), of: (i) in the case of a person with 5 fingers (including thumb) on one hand, any 3 of those fingers, or (ii) in the case of a person with only 4 such fingers, any 2 of those fingers, or (iii) in the case of a person with less than 4 such fingers, any one of them or, as the case may be, the one remaining finger, where none of the person’s fingers was subject to any degree of cold-induced, episodic blanching of the skin prior to the person’s employment in an occupation described in the third column in relation to this paragraph, or (b) significant, demonstrable reduction in both sensory perception and manipulative dexterity with continuous numbness or continuous tingling all present at the same time in the distal phalanx of any finger (including thumb) where none of the person’s fingers was subject to any degree of reduction in sensory perception, manipulative dexterity, numbness or tingling prior to the person’s employment in an occupation described in the second column in relation to this paragraph, where the symptoms in paragraph (a) or paragraph (b) were caused by vibration. |
Tools and processes which are associated with significant exposure to hand transmitted vibration including any hand-held, hand-guided or hand-fed, powered machine (e.g. pneumatic, hydraulic, electric (wired or battery) or internal combustion engine) that: a) is fitted with an abrasive or polishing attachment for the purpose of material removal (e.g. grinders, sanders) or finishing (e.g. polishers including floor polishers); or, b) is fitted with an attachment such as a cord (e.g. strimmer), blade (e.g. jig saw, cut-off saw, hedge trimmer, brush cutter, etc.) or cutting bit (e.g. woodworking machine or router) for the purpose of cutting, trimming or removing material; or, c) is fitted with an attachment such as a drill bit (e.g. rotary hammer) vibrating needles (e.g. needle scaler), scabbling head (e.g. scabbler), tines or spikes (e.g. aerator, scarifier), chisel, pick, spade (e.g. breaker, demolition hammer) for the purposes of making a hole in, or through, or otherwise breaking or removing material; or, d) is fitted with a rotating socket, driver bit or other attachment for the purpose of fastening or unfastening a component (e.g. wrench, ratchet, nut runner, impact driver, rivet gun, etc.); or, e) is fitted with a ram, plate or roller for smoothing or compaction of material (e.g. plate compactor, trench rammer, sand rammer, concrete screeding machine); or, f) which propels or expels a fluid (air or water) for the purposes of cleaning or moving dust, dirt and debris (e.g. leaf blower, water jetting lance); or, (g) which has a vibratory action for the removal of air from concrete (e.g. concrete poker). |
Note. An operator may also be at risk of developing HAVS if they grip a workpiece, tool or component as it is worked on or impacted by a machine (e.g. pedestal grinder, polishing machine, drop forge, spring hammer, bucking bar, shoe pounding machine).
67. In its role of supporting the operation of the Scheme the Council will assist with the preparation of operational guidance on the list of tools, industries and occupational history taking to assist Decision Makers and medical assessors. A non-exhaustive and alphabetical list of industries where HTV exposure is common is shown in Appendix 6.
68. The Council will continue to review both epidemiological and exposure data and, where appropriate, add further to this extended list.
Prevention
69. Guidance for employers is outlined in HSE guidance document L140. Set requirements for the control of exposure to hand-arm vibration are prescribed by EAV and ELV. The risks from HTV can be minimised by good work practices and where possible tasks that involve exposure to HTV should be eliminated or if not possible reduced as far as is reasonably practicable. Further information can be obtained from the HSE website.
References
Akesson I, Balogh I, Skerfving S. Self reported and measured time of vibration exposure at ultrasonic scaling in dental hygienist. Applied Ergonomics 2001; 32 (1) 47-51
Bovenzi, Massimo, Christopher J. Lindsell, and Michael J. Griffin. Acute Vascular Responses to the Frequency of Vibration Transmitted to the Hand. Occupational and Environmental Medicine 2000;57:422-30.
Bovenzi, M., et al., Frequency weightings of hand-transmitted vibration for predicting vibration-induced white finger. Scandinavian Journal of Work Environment & Health, 2011. 37(3): p. 244-252.
Bovenzi, M., Epidemiological Evidence for New Frequency Weightings of Hand-Transmitted Vibration. Ind Health, 2012. 50: p. 377-387. Bovenzi M, Pinto I, Picciolo F. Risk assessment of vascular disorders by a supplementary hand-arm vascular weighting of hand-transmitted vibration. Int Arch Occup Environ Health. 2019;92(1):129-139.
Burström L, Hagberg M, Lundström R, Nilsson T. Relationship between hand-arm vibration exposure and onset time for symptoms in a heavy engineering production workshop. Scand J Work Environ Health. 2006 Jun;32(3):198-203. doi: 10.5271/sjweh.999.
Department for Work and Pensions. Vibration White Finger. Report by the Industrial Injuries Advisory Council. Command Paper 8350. London: HMSO: September 1981.
Department for Work and Pensions. Hand-arm Vibration Syndrome (Vascular and Neurological Components Involving the Fingers and Thumb). Report by the Industrial Injuries Advisory Council. Command Paper 2844. London: HMSO:May 1995.
Department for Work and Pensions. Hand-arm Vibration Syndrome. Report by the Industrial Injuries Advisory Council. Command Paper 6098. London: HMSO:July 2004.
Department for Work and Pensions. Dupuytren’s contracture due to hand transmitted vibration. Report by the Industrial Injuries Advisory Council. Command Paper 8860 London: HMSO: May 2014.
Department for Work and Pensions. Noise, occupational deafness and Industrial Injuries Disablement Benefit: IIAC position paper 38, Report by the Industrial Injuries Council. London: HMSO, September 2017.
Department for Work and Pensions. Hand-arm vibration syndrome and risk from motorcycle handlebars: Information note. London: HMSO, 2017.
Department for Work and Pensions. A review of the assessment and objective testing for the vascular component of hand-arm vibration syndrome (HAVS). Report by the Industrial Injuries Advisory Council Position Paper 43. London: HMSO, July 2019
Dong RG, Welcome D E, McDowell TW, Wu JZ. Biodynamic response of human fingers in a power grip subjected to a random vibration. Journal of Biomechanical Engineering 2004. 126(4): 447-57.doi: 10.1115/1.1784479. Dong RG, Welcome DE, Wu JZ. Frequency weightings based on biodynamics of fingershand-arm system. Ind Health. 2005 Jul;43(3):516-26. doi: 10.2486/indhealth.43.516. PMID: 16100928.
Garner R, Kumari R, Lanyon P, Doherty M, Zhang W. Prevalence, risk factors and associations of primary Raynaud’s phenomenon: systematic review and meta-analysis of observational studies. BMJ Open. 2015 Mar 16;5(3):e006389. doi: 10.1136/bmjopen2014-006389
Gerhardsson L, Balogh I, Hambert PA, Hjortsberg U, Karlsson JE. Vascular and nerve damage in workers exposed to vibrating tools. The importance of objective measurements of exposure time. Appl Ergon. 2005 Jan;36(1):55-60.
Griffin MJ. Handbook of human vibration. Published: Academic Press, London, 1990 pp 660. ISBN: 0-12-303040-4.
Griffin MJ, Bovenzi M, Nelson CM. Dose-response patterns for vibration-induced white finger. Occup Environ Med. 2003;60(1):16-26. doi:10.1136/oem.60.1.16
Griffin M.J. Negligent exposures to hand-transmitted vibration. Int Arch Occup Environ Health. 2008 81, 645-659.
Health and Safety Laboratory. A critical review of evidence related to hand-arm vibration syndrome and the extent of exposure to vibration. Sue Hewitt, Howard Mason, HSL: RR1060 Research Report 2015.
Health and Safety Laboratory. Survey of noise emission and risk information supplied with a range of work machinery HSL: RR 962 Research Report 2013.
Health and Safety Executive. Control of vibration at Work Regulations 2005, L140 (2nd ed) ISBN 9780717665655
Health and Safety Executive. Hand-arm vibration: Inspection and Enforcement Guidance. 2020
International Organization for Standardization (ISO). Mechanical vibration – Measurement and evaluation of human exposure to hand-transmitted vibration. Part 1: General requirements. ISO 5349-1. Geneva: ISO, 2001.
International Organization for Standardization (ISO). Mechanical vibration – Measurement and evaluation of human exposure to hand-transmitted vibration. Part 2: Practical guidance for measurement at the workplace ISO 5349-2. Geneva: ISO, 2001.
International Organization for Standardization (ISO). Mechanical vibration -Measurement and evaluation of human exposure to hand transmitted vibration-Supplementary method for assessing risk of vascular disorders ISO/TR 18570:2017.
Krajnak K, Riley DA, Wu J, McDowell T, Welcome DE, Xu XS, Dong RG. Frequency-dependent effects of vibration on physiological systems: experiments with animals and other human surrogates. Ind Health. 2012;50(5):343-53. doi: 10.2486/indhealth.ms1378.
Lawson IJ. Is carpal tunnel syndrome caused by work with vibrating tools? Occup Med (Lond) 2020;70:8–10.
Miwa, Evaluation methods for vibration effect. Part 3: Measurement of thresholds and equal sensation contours on hand for vertical and horizontal vibrations. Industrial Health, 1967; 5: 213-220.
Montracon Ltd -v-Whalley [2005] EWCA CIV 1383 (21 NOVEMBER 2005) Court of Appeal.
Palmer KT, Griffin MJ, Sydall H, Pannett B, Cooper C, Coggon D. Prevalence of Raynaud’s phenomenon in Great Britain and its relation to hand transmitted vibration: a national postal survey Occup Environ Med 2000; 57: 448-452
Palmer KT, Haward B, Griffin MJ, Bendall H, Coggon D. Validity of self reported occupational exposures to hand transmitted and whole body vibration. Occup Environ Med. 2000;57(4):237-241. doi:10.1136/oem.57.4.237
VIBRISKS. Michael J. Griffin M J, Bovenzi M. Risks of Occupational Vibration Exposures. 2007; Annex 1 to Final Technical Report, Protocol for epidemiological studies of hand-transmitted vibration: Appendix 6 Alternative measures of vibration dose.
Appendix 1
A11. Extract from Current Prescribed Disease List
Type of job – Any job involving:
a. the use of hand-held chain saws on wood*; or
b. the use of hand-held rotary tools in grinding or in the sanding or polishing of metal, or the holding of material being ground, or metal being sanded or polished, by rotary tools; or
c. the use of hand-held percussive metalworking tools, or the holding of metal being worked upon by percussive tools, in riveting, caulking, chipping, hammering, fettling or swaging; or
d. the use of hand-held powered percussive drills or hand-held powered percussive hammers in mining, quarrying, demolition, or on roads or footpaths, including road construction; or
e. the holding of material being worked upon by pounding machines in shoe manufacture.
*From 1 October 2007 the occupational prescription in process (a) changed from the use of handheld chain saws in forestry to their use on wood: Other employees who use a chainsaw to cut down trees, for example, railway labouring gangs, are covered by the prescription provided the use of the tool is more than incidental to the employment.(SS (II) (PD) Regs, Sch 1, Part 1; 2 Secretary of State v Davis)
Appendix 2
Extract from HSE web site: Worried about your hands?
Tasks and industries
Which jobs and industries are most likely to involve hand-arm vibration? Jobs requiring regular and frequent use of vibrating tools and equipment and handling of vibrating materials are found in a wide range of industries, for example:
- building and maintenance of roads and railways;
- construction
- estate management (eg maintenance of grounds, parks, water courses, road and railside verges)
- forestry
- foundries
- heavy engineering
- manufacturing concrete products
- mines and quarries;
- motor vehicle manufacture and repair
- public utilities (eg water, gas, electricity, telecommunications);
- shipbuilding and repair
Tools
What kinds of tools and equipment can cause ill health from vibration? There are hundreds of different types of hand-held power tools and equipment, which can cause ill health from vibration. Some of the more common ones are:
- chainsaws
- concrete breakers/road breakers
- cut-off saws (for stone etc)
- hammer drills
- hand-held grinders
- impact wrenches
- jigsaws
- needle scalers
- pedestal grinders
- polishers
- power hammers and chisels
- powered lawn mowers
- powered sanders
- scabblers
- strimmers/brush cutters
Appendix 3
List of occupational exposures recommended for prescription Cm 2844 (1995).
Percussive metal-working tools
Riveting tools (hammers and dollies)
Caulking tools
Chipping hammers
Fettling tools
Drilling tools (including hammer drills)
Pneumatic hammers
Impact wrenches
Staging tools
Metal-shearing and cutting machines
Impact screwdrivers
Grinders and other rotary tools
Pedestal grinders
Hand-held portable grinders (including angled grinders) sanders and polishers
(including floor polishers)
Flex-driven grinders
Flex-driven polishers (including floor polishers)
Rotary burring tools
Rotary tagging machines
Readers
Fixed linishers
Engraving pens
Stone working, mining, road construction and road repair
Hammers (including jack-hammers and kango-hammers)
Rock (etc) drills
Road breaking tools
Road reinstating tools
Forest, garden and wood-working machinery
Chain saws
Anti-vibration chain saws
Electrical driven screwdrivers
Brush saws
Mowers and shears
Hardwood cutting machinery
Barking machines
Stump grinders
Hedge trimmers
Rotary hoes
Hand-held or hand fed circular saws
Other processes and tools
Drain suction machines
Nut runners
Pounding-up (pound seat) machines
Concrete-vibrating pokers
Concrete vibro-thickeners
Concrete levelling vibrotables
Jigsaws
Scabblers
Vibratory rollers
Appendix 4 Vibration nomenclature
Assessing Vibration
Vibration is an oscillatory motion (either a sine wave or multiple wave complex which can be measured by a number of parameters including:
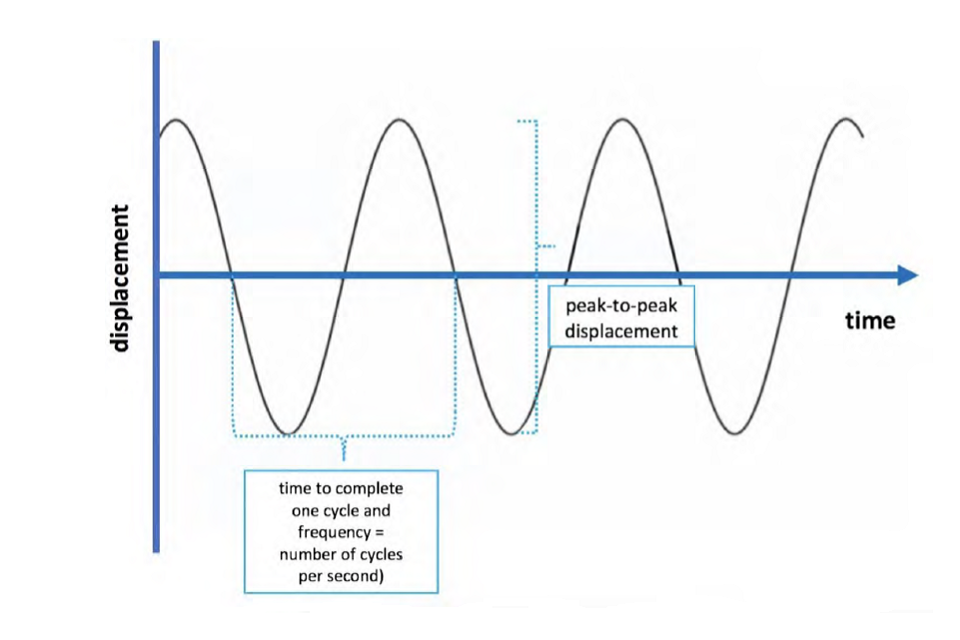
- displacement in metres (m). Occurs in three orthogonal axis X,Y,Z.
- speed of the wave or its velocity, v (ms-1)
- acceleration, a (ms-2) i.e., the rate of change in velocity.
- Frequency, f or wave cycles per second measured in Hertz (between 1 to 1000 Hz)
An acceleration value can be recorded by accelerometers attached to tools or by a hand adaptor and is the usual practical way of assessing the magnitude of vibration. This ‘average’ level is recorded during a time period as a root mean square (rms) level in meters per second (ms-2) and represented by the term ahv (acceleration, hand, vibration).
This acceleration value is referred to as the vibration magnitude and should be assessed in accordance with International Standard, ISO 5349-1. As some frequencies are thought to be more damaging a frequency weighting (Wh) correction is also applied to the measurements. Vibration occurs in 3-axis (x,y,z) and as each is presumed to be equally damaging, a vector sum of the three axis is calculated (ahv = √ ahvx2 + ahv2 + ahvz2). The time each tools is used recorded and the daily vibration magnitudes is calculated
This daily vibration magnitude is referred to as A(8) in ms-2 where:
A(8) = ahv√T/T0 where T is the total daily duration of exposure to vibration and T0 an 8 hour equivalence.
International Standard ISO 5349-1
International Standard ISO 5349-1 was developed by a subcommittee of a Technical Committee ISO/TC 108 / SC4. It covers the measurement and evaluation of hand transmitted vibration. The standard superseded a previous version published in 1986. The latter used latency data from groups of workers working full time with a prevalence of symptoms of greater than 50% and extrapolated to 40,30,20 and 10%. The revised standard published in 2001 restricted the dose-response relationship to a prevalence of 10 % finger blanching to ‘limit the potential for inappropriate use of the relationship.’
Annex C of the standard shows the relationship between A(8) and duration exposure in years (Y) using frequency weighting Wh and based epidemiological studies of workers using vibrating tools (frequency range 30 Hz to 50 Hz) that produces 10% finger blanching in a group and is represented by the equation: Y10% [31.8] A(8)-1.06. The equation adopted for the model used in this command paper is an approximation of this represented by the equation Y10% ≈ 30/A(8). The standard notes that acceleration values derived from these studies were the dominant, single-axis, frequency-weighted component acceleration and refers the use of a multiplying factor to convert to a total vibration value. Annex C of the standard also emphasises that it should not be used to predict finger blanching in any individual of a group of vibration exposed.
Annex D of the standard acknowledge that the probability of a worker developing HAVS depends on both ergonomic and individual susceptibility, any pre-existing diseases and conditions, and various work-related, environmental and personal factors.
ISO Technical Report, ISO/TR 18570-2017
ISO/TR 18570:2017 was prepared to provide guidance on a supplementary method for measuring and evaluating hand-transmitted vibration exposure and VWF with the intention of facilitating future research on hand-arm vibration and not as an alternative to ISO 5349‑1. An alternative frequency weighting (Wp) is proposed based on the biodynamic, pathophysiological and epidemiological evidence suggesting that hand and finger tissue damage occurs at frequencies > 100 Hz. Annex A of the Technical Report proposes a ‘daily exposure threshold’ at which onset of symptoms of finger blanching may be expected to occur at an estimated exposure value for a working day, Ep,d of 1750 ms-1.5 (corresponding to Ap(8) of about 10.3 ms-2).
Appendix 5 HAVS and PDA11
Diagnosing HAVS using the criteria in paragraph 20 is only one step in the process of assessment in relation to PD A11. The medical assessor is also required to answer the ‘occupation’ question by taking a… ‘Full occupational history, including the nature of tools used, the percentage of the day spent using these tools, and the length of time in years using these tools.’ (MED-IIBHB~002 page 55).
The onset, progression and severity of symptoms also needs assessing in relation to the vibration exposure (the onset and progression of symptoms was reviewed by the the Council in 2019, Position Paper 43). Increasing intensity and duration of exposure may lead to onset and increasing severity of HAVS but the relationship is not a linear one. Cases can occur very rapidly with high magnitudes of exposure, show plateauing in severity and have minimal progression even with long term exposure.
HAVS can be regarded as a ‘more or less’ condition and the ‘diagnostic’ question in PD A11 is only effectively satisfied when the disease has reached the severity outlined in the prescription. Making a judgement on whether there has been sufficient vibration exposure in relation to onset and progression, particularly when a variety of tools are used, may not be straightforward but nevertheless should always be assessed in conjunction with the clinical history.
HAVS is also non-deterministic is the sense that there is no clear cut threshold of exposure above which the condition is likely to occur. A putative vibration magnitude A(8) of 1 ms-2 (Annex C ISO 5349-1) below which harmful effects are not thought to occur has been accepted in some employers liability cases. Any putative threshold level of vibration dose should not be confused with HSE action level (EAV) which accepts a 10% level of risk.
Tool vibration magnitudes may be obtained by measurements, tool supplier information on emissions or from published data e.g. HSE 75th percentile values. However, there are a number of variables other than these assumed vibration magnitudes that can potentially affect the dose-response relationship:
- range in vibration magnitudes for the same tool
- intermittency of exposure
- impulsive or impact vibration
- workpiece hardness
- workplace maintenance of tools
- task ergonomic factors
- individual susceptibility
In addition daily, yearly and intermittency of vibration exposure can be influenced by recall bias.
For these reasons the medical assessors should not rely on a fixed threshold of an assumed vibration magnitude, set number of years of exposure or the product of these when making their judgements. As with current practice each case is assessed on an individual basis combining the clinical history with a detailed occupational history.
The conclusion in this command paper is that using the Y10% model, (based on ISO 5349-1) as a surrogate measure to determine the sufficiency of exposure on an individual basis would be inappropriate. However, the Council will produce guidance notes to aid the medical assessment process with the aim of complementing the clinical and occupational history. They will include the range and types of tools recommended in paragraph 67 (some of which may be unfamiliar to Decision Makers and medical assessors), vibration magnitudes ranges and workplace tasks. The intention of the guidance is not as a replacement for the current assessment process nor as a means of setting a vibration dose threshold.
The following hypothetical example deploying a range of vibration magnitudes for the same tool (HSE ‘lower’ 10th and ‘upper 90th percentile values of vibration magnitudes) demonstrates the potential flaw when applying the Y10% too rigidly to an individual assessment.
Pedestal grinders (assumed range: ‘lower’ 2 ms-2 and ‘upper 11 ms-2 percentile values of vibration magnitudes).
Two pedestal grinders working 8 hour days. With breaks and some hand held polishing factored in to regular overtime hours the A(8) values were calculated as lower 2.5 ms-2 for grinder A and upper 12 ms-2 for grinder B.
Grinder A develops sensory symptoms after seven years and vascular symptoms after eight years. Symptoms progressed rapidly after that, and a PD A11 claim is initiated after 10 years from the start of exposure. The vascular symptoms satisfied the severity criteria for the diagnostic question. Applying Y10% (30/A(8)) would mean a theoretical onset of vascular symptoms only after 12 years at these exposures.
Grinder B develops sensory symptoms after 5 years of exposure and mild vascular symptoms after 8 years which initially worsen but plateau for a number of years. A PD A11 claim is initiated at 16 years after the start of exposure and satisfies the severity criteria for the diagnostic question. Applying Y10% (30/A(8)) would mean a theoretical onset of vascular symptoms after two and a half years of exposure.
Despite both satisfying the diagnostic question applying Y10% as a fixed cut off would mean case A would fail to satisfy the occupation question whereas B would satisfy it.
Appendix 6
Industries where hand transmitted vibration exposure is common (non-exhaustive)
Aggregates
Aircraft manufacturer and repair
Boat building and repair
Boiler making
Building maintenance
Civil engineering
Coach building
Concrete
Construction
Diamond drilling
Demolition
Engineering
Fabrication
Forestry
Foundry
Grounds maintenance
Ground work
Highways maintenance
Horticulture
Joinery
Manufacturing
Metal fabrication
Mining
Motor vehicle manufacture and repair
Spray painting
Steel fabrication
Tree surgery
Quarrying
Rail track construction and maintenance
Rail vehicle manufacture and maintenance
Road construction and maintenance
Shipbuilding and ship repair
Steel manufacturing
Stone masonry
Utilities
Waste services
Welding
Woodworking
External experts consulted when preparing this report
Tohr Nilsson, Associate Professor Occupational and Environmental Medicine, Department of Public Health & Clinical Medicine, Umeå University, Umeå, Sweden
Professor Massimo Bovenzi, Professor of Occupational Medicine, University of Trieste, Italy.
Dr Chris Nelson, Principal Consultant (Noise & Vibration), Finch Consulting, Leicestershire, UK.
Ms. Sue Hewitt, Senior Consultant, Finch Consulting, Leicestershire, UK.
-
Σ means ‘the sum of’ ↩