IIAC annual report: 2022 to 2023
Published 14 September 2023

© Crown copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/iiac-annual-report-2022-to-2023/iiac-annual-report-2022-to-2023
© Industrial Injuries Advisory Council copyright 2023
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated.
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at: Industrial Injuries Advisory Council
Any enquiries regarding this publication should be sent to us at: [email protected]
Foreword
Like many committees, IIAC has now settled into a pattern of using a hybrid format for all its regular meetings, with subgroup meetings on specific topics being mainly held online.
The Council has reviewed and evaluated several major occupational health issues that has resulted in publication of two Command papers and a Position paper, with a further Command paper expected to be published in autumn 2023.
Once again, a major part of the work of the Council this year has been the continuing evaluation of the impact of the Covid-19 pandemic and the potential risks to workers. This year there were a large number of published studies, and other relevant data which required continual monitoring and evaluation and involved the Members and the Secretariat in considerable amount of work. This resulted in the publication of a Command paper recommending prescription for Health and Social Care workers who developed one or more of five serious pathological complications following COVID-19. On-going work in this area includes consideration of potential expansion of the recommendations to include other occupations, particularly the transport and education sectors, and monitoring data on the longer-term consequences of COVID-19, such as Post-Covid syndrome.
The other Command papers address two older prescriptions, Pneumoconiosis and Hand Arm Vibration Syndrome, with the aim of ensuring that these are clearer and more accessible to both claimants and administrators. An important element of the revisions for both these issues is to ensure that they now allow a wider and more up-to-date range of exposure scenarios.
A commissioned review of occupation and COPD, lung cancer and other respiratory diseases is underway and it is expected that this will highlight some important areas for the Council to evaluate. The Council are aware that IIAC has never specifically addressed the issue of women’s occupation and ill-health. Both occupationally related malignant and non-malignant disease in women is expected to be a focus of the Council’s work in future.
I would like to thank all the Council members, the HSE, MOD and other observers, the Secretariat and members of the Department for their hard work and dedication this year and am reassured that this will continue in future.
Dr Lesley Rushton
IIAC Chair
Introduction
The Industrial Injuries Advisory Council (IIAC) is a non-departmental public body (NDPB) established under the National Insurance (Industrial Injuries) Act 1946, which came into effect on 5 July 1948. The Council provides independent advice to the Secretary of State for Work and Pensions in Great Britain and the Department for Communities (DfC) in Northern Ireland on matters relating to Industrial Injuries Disablement Benefit and its administration. The historical background to the Council’s work and its terms of reference are described in Appendix A and Appendix B respectively.
The Role of the Council
The statutory provisions governing the Council’s work and functions are set out in sections 171 to 173 of the Social Security Administration Act 1992 and corresponding Northern Ireland legislation. The Council has three main roles:
- to consider and advise on matters relating to Industrial Injuries Disablement Benefit (IIDB) or its administration referred to it by the Secretary of State for Work and Pensions in Great Britain or the DfC in Northern Ireland.
- to advise on any other matter relating to IIDB or its administration.
- to consider and provide advice on any draft regulations the Secretary of State proposes to make on IIDB or its administration.
IIAC is a scientific advisory body and has no power nor authority to become involved in individual cases nor in the decision-making process for benefit claims. These matters should be taken up directly with the Department for Work and Pensions, details of which can be found on the GOV.UK website.
Composition of the Council
IIAC usually consists of around seventeen members, including the Chair. It is formed of independent members with relevant specialist skills, representatives of employees and representatives of employers. The independent members currently include medical and scientific experts and two lawyers. Membership of the Council during 2022/23 is described in Appendix C.
Legislation leaves it to the Secretary of State to determine how many members to appoint but requires that IIAC includes an equal number of representatives of employees and employers (Social Security Administration Act 1992, Schedule 6).
Conditions for ‘Prescribing’ Diseases
Much of the Council’s time is spent considering which diseases, and the occupations that cause them, should be included in the list of diseases (‘prescribed diseases’ (PD)) for which people can claim IIDB.
The conditions which must be satisfied before a disease may be prescribed in relation to any employed earners are set out in section 108(2) of the Contributions and Benefits Act 1992. This requires that the Secretary of State for Work and Pensions should be satisfied that the disease:
- ought to be treated, having regard to its causes and incidence and any other relevant considerations, as a risk of occupations and not as a risk common to all persons; and
- is such that, in the absence of special circumstances, the attribution of particular cases to the nature of the employment can be established or presumed with reasonable certainty.
In other words, a disease can only be prescribed if the risk to workers in a certain occupation is substantially greater than the risk to the general population and the link between the disease and the occupation can be established in each individual case or presumed with reasonable certainty.
In some instances, recommendations for prescription of a disease can be made on the basis of clinical features which confirm occupational causation in the individual claimant. Increasingly, however, the Council has to consider diseases which do not have clinical features that enable the ready distinction between occupational and non-occupational causes (e.g., chronic obstructive pulmonary disease, which can be caused by tobacco smoking as well as having occupational causes). In these circumstances, in order to recommend prescription, IIAC seeks epidemiological evidence that the disease can be attributed to occupation on the balance of probabilities under certain defined exposure conditions (generally corresponding to evidence from several independent research reports that the risk of developing the disease is more than doubled in a given occupation or exposure situation), and thus is more likely than not to have been caused by the work. In 2015, the Council prepared a lay person’s guide to prescription, which was published on the GOV.UK website.
Research
The Council relies on research carried out independently, which is published in the specialist medical and scientific literature. IIAC does not have its own research budget to fund medical and scientific studies (other than limited funding from DWP for the occasional commissioning of reviews). When IIAC decides to investigate a particular topic its usual practice is to ask other bodies and interested parties to submit any relevant research in that field. IIAC has a sub-committee, the Research Working Group (RWG), which meets separately from the full Council to consider the scientific evidence in detail. The Council’s secretariat includes a scientific adviser who researches and monitors the medical and scientific literature in order to keep IIAC abreast of developments in medical and scientific research and to gather evidence on specific topics which the Council decides to review.
In March 2015, the Council published some informal guidance on how it reviews and reports on published literature, particularly epidemiological studies, to provide evidence for potential prescription for IIDB.
Key achievements of 2022/2023
Command Papers[footnote 1]
- occupational impacts of COVID-19, published November 2022
- a review of the assessment of vibration exposure in Prescribed Disease A11 (PD A11), Hand Arm Vibration Syndrome (HAVS), published July 2023.
- review and update of the prescription for prescribed disease PD D1, pneumoconiosis, due to be published autumn 2023
Some of these are described below in the section on work undertaken in 2022/23.
Position Papers[footnote 2]
No position papers were published 2022/2023; however, the following paper was published in July 2023:
- limitations of epidemiology when investigating occupations with a potential for significant vibration exposure and PD A11, Hand-Arm Vibration Syndrome.
This is described below in the section on work undertaken in 2022/23.
Information Notes[footnote 3]
Dupuytren’s contracture: clarification of intention and amendment of the prescription, published April 2023
Regulations proposed by the Secretary of State
The law requires that draft regulations proposed by the Secretary of State which concern the Industrial Injuries Disablement Benefit Scheme are referred to the Council for its advice and consideration. There were no regulations put to the Council for consideration in 2022/2023.
Stakeholder Engagement
The Council will hold a hybrid public meeting on 6 July 2023 in Cardiff and online. Proceedings will be published when available.
Topics to be discussed include:
- COVID-19 and occupation
- Reviewing occupations for PD A11 (Hand Arm Vibration Syndrome (HAVS))
- IIAC’s proposed revision of PD D1 (Pneumoconiosis, silicosis, asbestosis)
- Neurodegenerative diseases in professional sportspeople
- IIAC commissioned review into respiratory diseases
Appointments
During the year the terms of office of three members came to an end. The Chair was reappointed for two years from 1 April 2023. A recruitment campaign was begun to appoint new members to replace employee and employer member representatives and independent members, with appointments taken up in January 2023.
IIAC Meetings
Following the lifting of COVID-19 restrictions, meetings of the full Council and RWG have taken place using a hybrid approach where some members have attended in person and others joined the meetings via video conference, facilitated by the secretariat.
Summary of work undertaken in 2022/2023
The Council continued to undertake its advisory function effectively and the work undertaken is summarised below. However, the majority of the Council’s time was once again taken up by evaluation of the occupational impact of COVID-19.
COVID-19 and occupation – ongoing monitoring of the emerging data for other occupations.
Although most people infected with SARS-CoV-2 experience relatively mild or short-term symptoms, a small proportion report longer-term symptoms that lead to persisting loss of function and disability.
There is a large body of consistent supporting evidence showing that, for Health and Social Care Workers, whose work brings them into frequent close proximity to patients or clients, there is a significantly increased risk of infection, subsequent illness, and death. The Council therefore felt that there was sufficient evidence to recommend prescription for these workers in command paper CP740 ‘COVID-19 and Occupational Impacts’ and it identified robust evidence for the prescription of serious pathological complications following COVID-19 which have been shown to cause persistent impairment and loss of function in some people.
These are:
- persisting pneumonitis or lung fibrosis following acute COVID-19 pneumonitis;
- persisting pulmonary hypertension caused by a pulmonary embolism developing between 3 days before and 90 days after a diagnosis of COVID-19;
- Ischaemic stroke developing within 28 days of a COVID-19 diagnosis;
- Myocardial infarction developing within 28 days of a COVID-19 diagnosis;
- symptoms of Post Intensive Care Syndrome following ventilatory support treatment for COVID-19.
There was less robust and consistent evidence for other occupational sectors although the Council noted some evidence of increased risk of infection and mortality in occupations such as bus and taxi drivers and in those who worked in education. The Council concluded, however, that currently, the evidence was of insufficient quantity and quality to recommend prescription for these occupations. Since the publication of the Command paper, more evidence has become available for transport workers and those working in educational sectors and an evaluation of workers in these sectors will be reported in a subsequent paper.
A review of the assessment of vibration exposure in Prescribed Disease A11, Hand Arm Vibration Syndrome (HAVS)
Hand-Arm Vibration Syndrome (HAVS) can occur following exposure to Hand Transmitted Vibration (HTV) causing episodic finger blanching (the vascular component) and/or symptoms of numbness, tingling, reduced sensation and loss of dexterity of the fingers (the sensorineural component). The current prescription is defined in terms of HTV occurring following the use of a given list of tools and processes. The Industrial Injuries Advisory Council (IIAC) became aware that the current list diverged from other lists, including from the Health and Safety Executive.
The Council investigated the availability of epidemiological studies for extending the prescribed occupations for HAVS and found that there was very little. The Council therefore decided to explore two alternative approaches and these were reported in a command paper, CP 868 ‘Hand-arm vibration syndrome and assessment of vibration exposure’ published July 2023.
The first involved a review of the assessment of vibration magnitudes, exposure response relationships and risk prediction modelling based on International Standard, ISO 5349-1. A draft procedure for implementing this approach was developed, shared with external experts and departmental representatives and tested to see if was practicable. Although this process demonstrated this approach could potentially be used to identify additional tools or processes, it became evident during the review and from feedback received that there were a number of practical drawbacks when applied to assessing individual exposure.
The second approach entailed consultation with external experts on the feasibility of an extension to the list based on their knowledge and experience of vibrating tools and the potential to develop hand arm vibration syndrome. The Council felt that this approach was more suitable and following further consultation with external experts an extended list of vibrating tools was compiled to replace the existing list. The list of tools is separated by categories with examples of specific tools in each.
The epidemiological evidence for HAVS in several occupations that are not included in the current prescription were reviewed and a position paper, ‘Limitations of epidemiology when investigating occupations with a potential for significant vibration exposure: IIAC position paper 49’ reporting the findings was published separately in July 2023.
Review and update of the prescription for prescribed disease PD D1, pneumoconiosis.
The current prescription for pneumoconiosis dates back in part over 100 years and has not undergone any major revision for almost 80 years. In that time the causes of the disease and the diagnostic techniques have changed substantially. The current prescription can be difficult to navigate for both claimants and administrators. In addition, the specified occupations are largely historic and do not include those where current exposures may occur, particularly for silica. Following considerable deliberations and the consultation of external respiratory disease experts, the Council recommends that the disease considered in the revised prescription should be ‘pneumoconiosis’ without any further qualification and that work involving exposures to the following should be included as potential causes of pneumoconiosis for the purpose of PD D1:
a. Asbestos b. Coal or coal mine dust c. Silica-containing dusts d. Metal dusts: aluminium, beryllium, cobalt, indium tin oxide, rare earth metals, and tungsten carbide
The clinical and radiological features of pneumoconioses can be similar to those of other lung diseases and there are often alternative diagnoses and treatments. IIAC therefore expects that a specialist clinical opinion should normally be obtained before an application for IIDB for pneumoconiosis is considered.
IIAC recommends that awards of benefit for pneumoconiosis should be brought into line with those for other conditions, with no automatic award on diagnosis irrespective of the actual disability. Claims for comorbid chronic obstructive pulmonary disease (COPD) should now be considered separately. In addition, awards for complicating tuberculosis and non-tuberculous mycobacterial infection should be restricted to pneumoconioses associated with silica exposures.
No changes are proposed to the extent of exposure needed to establish a diagnosis for any of the prescribed exposures or to the assessment of disability.
These recommended changes to prescription PD D1 will be set out in a command paper which is expected to be laid before Parliament and published online in autumn 2023.
Evidence update of the relationship between occupational exposures and selected malignant and non-malignant respiratory disease.
Some of the current prescriptions for respiratory diseases have been re-evaluated more than once since their inception many decades ago. However, they do not always reflect occupations and modern work practices where exposure may occur more frequently than in the past, such as in the construction industry and/or new products are now in use such as the use of artificial/composite stone which often contains a high percentage of quartz.
Currently COPD is only prescribed in relation to coal mining. However, there is a large literature in many different industries showing consistent associations from several occupational-related exposures with increased risk of death or incidence of COPD, for example: work in construction, tunnelling, manufacture of ceramic fibres, iron and steel foundry work, cotton manufacture, grain handling, welding, and agriculture.
For lung diseases, a particular challenge for prescription is how to take account of important confounding exposures, and in particular, smoking. This is illustrated in the current prescription for COPD and coal mining, which was based on data that included both smokers and non-smokers; smoking habits of claimants are thus ignored.
The Council appointed the Institute of Occupational Medicine (IOM) to carry out the review and work has progressed.
Following discussions with the Council, 6 priority exposure/disease combinations were agreed for further consideration:
- Silica & COPD
- Silica & lung cancer
- Cleaners & nurses and COPD
- Farming/pesticide spraying & COPD
- Hexavalent chromium and lung cancer
- Asbestos and lung cancer.
Literature searches have been carried out and IOM are currently evaluating the results. Tables of evidence will be produced and reports for the exposure/disease combinations will be drafted. This will enable the Council to determine if changes to current prescriptions are required or if there is sufficient evidence to recommend new prescriptions.
Neurodegenerative brain disease in professional sportspeople
The Council received correspondence from a charity giving information about a former professional footballer for whom a Coroner had recorded a verdict of ‘death by an industrial disease’. A consultant neuropathologist found considerable evidence of trauma to the footballer’s brain likely to have been exacerbated by his profession. Evidence was submitted to support this claim and a request was made for IIAC to investigate the potential link to neurodegenerative disease (NDD) in professional football players. Subsequently, the Professional Footballers Association (PFA) wrote to the Council to ask it to look into the possible link. Following a review of NDD in rugby players, this prompted the Council to expand the investigation to include other sports.
This is a particularly complex topic to investigate: (i) it is not always possible to determine the key exposures and these vary between the different sports; (ii) the published literature often refers to ‘neurodegenerative disease’ whereas, in reality, there are several different disease conditions with differing morphology. It was decided to focus initially on amyotrophic lateral sclerosis (ALS or Lou Gehrig’s disease) and motor neurone disease (MND) as these appear to have positive signals in the literature. A number of review studies were identified and further literature search carried out. Members are currently evaluating the papers.
Other work carried out in 2022/2023
The Fire Brigades Union (FBU) contacted the Council following the publication of a study in Scottish firefighters which indicated higher than expected risks of several cancers. Members of the Council evaluated the methodology used in the paper to determine the risks in firefighters and contacted the author to ask for clarification of certain points. The response was helpful but raised further questions. The author was contacted again but the Council has yet to receive a response. Therefore, currently, it is unlikely the Council will deviate from its comprehensive review published in position paper 47 – firefighters and cancer but will keeping a watching brief on emerging evidence including any further details on the Scottish study.
Discussions were held to establish the priorities for the ongoing programme of work. A major question considered was women’s occupational health, which has never been specifically considered by the Council as a stand-alone topic. It was suggested to look at non-malignant diseases in women and reproductive conditions were considered to be relevant.
In order to understand the topic better, it was suggested that a scoping review be carried out and a short paper summarising the proposed approach was circulated in meeting papers. The other issue to consider was cancers in women and it was suggested to not consider breast cancer at this stage due to its complexity and potential involvement of non-occupational causes – this would probably warrant its own investigation. Asbestos and ovarian cancers may be evaluated.
Future Work of the Council
In addition to maintaining its reactive brief, the Council will continue with its horizon scanning of the recently published scientific research literature which will inform its work programme for 2023/2024.
Summary of sources and outcomes of IIAC investigations
IIAC continues to be committed to publishing statistics related to the sources and outcomes of investigations to improve transparency.
The information shown below illustrates the breakdown in sources of referrals made to the Council and the outputs of these investigations.
Figure 1: Source of IIAC investigations 2022-23
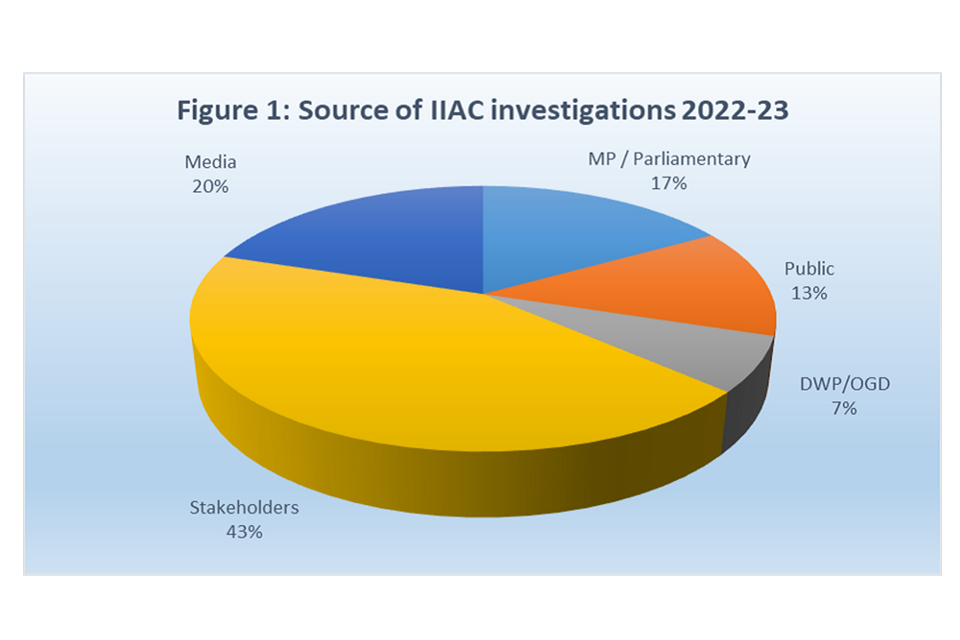
Figure 2: Outcomes of IIAC investigations 2022-23

Stakeholder Engagement
Networking activities
External experts
IIAC consults with external parties on a range of topics (acknowledged in written reports).
In the past year, experts have been consulted for the Council’s reviews of Pneumoconiosis and HAVS.
The Chair consulted with UKHSA to seek definitions for an outbreak and an incident to help inform the Council’s work relating to COVID-19.
External engagement /Public meeting
A public meeting is scheduled for 6 July 2023, to be held in Cardiff with the option for attendees to join online.
The Chair and a member attended a meeting of an All Party Parliamentary Group (APPG) on long-covid.
The Chair held discussions with Chief Medical Officer at Transport for London on COVID-19 impacts on transport workers.
A member spoke with the TUC on the findings of the joint report by the TUC and Long Covid Support into ‘Worker’s experience of long-covid’.
Members with respiratory expertise attended a meeting of the Group of Occupational Respiratory Disease Specialists (GORDS) to discuss the Councils review of pneumoconiosis.
The Chair and members attended a meeting with the PFA and the TUC to discuss NDD in footballers.
IIAC have reached out to the authors of a recent study of Scottish firefighters to ask for further details on how the study was conducted. An initial response was received and having reviewed it, sought further clarification from the authors. To date there has been no response. Follow-up will be sought after a reasonable period has been given to respond.
Initial discussions were held with the Institute for Occupational Medicine with a possibility of working together on a scoping review for selected non-malignant topics concerning women’s occupational health.
Calls for additional research, highlighting occupational risks for prevention
IIAC does not have its own research budget and its remit does not extend to commissioning primary research studies. Thus, IIAC must rely on published research when considering whether a disease and exposure warrant prescription. IIAC strives to identify robust evidence from the peer-reviewed scientific literature, but where such information is lacking will seek other avenues to provide information, such as approaching researchers directly to ask for additional analyses of, or further information about, their data.
The Council regularly makes calls for evidence to the wider scientific community via its site on gov.uk/iiac, the Society of Occupational Medicine’s newsletter and through a targeted approach to the occupational sectors involved.
Membership
Under the Social Security Administration Act 1992 (Schedule 6) the Secretary of State appoints a Chair and any other number of members as they may determine. Legislation requires that there shall be an equal number of persons to represent employers and employed earners.
Since April 2018 the IIAC chair receives an annual fee. However, the Chair and members of IIAC are not salaried. For each meeting they attend members receive a fee and reimbursement of travelling expenses and subsistence (where appropriate) in line with civil service arrangements.
IIAC members are required, at the start of each meeting, to declare any conflict of interest in relation to the business of the meeting. For transparency these are recorded in the minutes of meetings, and on a register of members’ interests, both of which are published on gov.uk/iiac.
Appointments and reappointments
Four new appointments and one reappointment were made during 2022-2023:
- Sally Hemming was appointed as an employer representative, Steve Mitchell as an employee representative, with Dr Richard Heron and Dr Sharon Stevelink appointed as independent members. All were appointed for five years from 3 January 2023.
- Dr Lesley Rushton, the IIAC Chair was reappointed for second term of two years from 1 April 2023.
All appointments are made through open, fair and transparent competition, complying with the Governance Code published by the Minister for the Cabinet Office in compliance with the Public Appointments Order in Council 2019.
Full details of IIAC membership throughout the year can be found at Appendix C.
Appendix A – Historical background to the Council’s work
The first Workmen’s Compensation Act passed in 1897 made no provision for industrial diseases. Subsequently, a Departmental Committee identified a need for additional statutory provision and a Schedule was added to the Workmen’s Compensation Act of 1906 listing industrial diseases for which compensation was available. Initially only six diseases were prescribed (anthrax, poisoning by lead, mercury, phosphorus, and arsenic, and ankylostomiasis) in respect of specific work processes. The 1906 Act also empowered the Home Secretary to add other diseases to the Schedule, though the criteria to be applied in doing so were not specified.
The Samuel Committee was appointed in 1907 to inquire into this and set out to identify diseases currently not covered by the Act which, firstly, caused incapacity for more than one week and, secondly, were so specific to the given employment that causation could be established in each individual case. Using these criteria, the Committee recommended that eighteen diseases should be added to the Schedule. Further diseases were added to the schedule later, but there were no significant changes to the scheme until the setting up of the Welfare State after the Second World War. By 1948 compensation was available for 41 diseases.
IIAC was established under the National Insurance (Industrial Injuries) Act 1946. Under this Act, which came into effect on 5 July 1948, a new Industrial Injuries Scheme was established, financed by contributions from employers, employees and the Exchequer. The State, through the Scheme, assumed direct responsibility for paying no-fault compensation for work related injury and diseases. The Council’s terms of reference, set down in the Act, were to advise the Minister on proposals to make regulations under the Act and to advise and consider such questions relating to the Act that the Minister might, from time to time, refer.
The 1946 Act also contained provisions for the prescription of diseases (section 55 of the 1946 Act, now section 108(2) of the Contributions and Benefits Act 1992). The Minister could prescribe a disease if he or she was satisfied that it ought to be treated as a risk of occupation and not as a risk common to the general population, and that the attribution of individual cases to the nature of the occupation could be established or presumed with reasonable certainty. An employee disabled by a prescribed disease would have a right to claim benefit under the Act.
In 1947 the Government appointed the Dale Committee. Part of its brief was to advise on the principles governing the selection of diseases for insurance under the National Insurance (Industrial Injuries) Act, having regard to the extended system of insurance which was about to be set up by the National Insurance Act 1948 and any other relevant considerations. The advice of the Dale Committee included proposals that a small specialised standing committee should be appointed by the Minister to consider the prescription of diseases specifically referred to it, to review periodically the schedule of prescribed diseases and to recommend subjects on which more research was needed. The Minister concluded that this was a suitable task for a newly established IIAC. In 1982 the Government widened the Council’s terms of reference allowing it to advise the Secretary of State on any matter relating to the Industrial Injuries Disablement Benefit Scheme or its administration.
Appendix B – Terms of Reference
Purpose and constitution
To advise the Secretary of State for Work and Pensions, the Medical Advice Team of the Department for Work and Pensions (DWP) and the Department for Communities in Northern Ireland on the Industrial Injuries Scheme.
The Social Security Administration Act 1992 sets out the Council’s remit. The Council exists to provide consideration and advice to the Secretary of State on matters relating to Industrial Injuries Disablement Benefit (IIDB) or its administration, and to consider any draft regulations the Secretary of State proposes to make in relation to that scheme. In particular this includes advising which diseases and occupations should give entitlement to Industrial Injuries Disablement Benefits.
Membership
The Council consists of a Chair appointed by the Secretary of State and such number of other members so appointed as the Secretary of State shall determine. Currently, independent members include specialists in occupational medicine, epidemiology, exposure measurement and the law. Legislation also requires an equal number of representatives from employers and employees.
Appointments shall be made by the Secretary of State or another Minister of the DWP as determined by the Secretary of State. Appointments shall be made in accordance with the Governance Code of Practice for public appointments published by the Cabinet Office which sets out the regulatory framework for public appointments processes within the Commissioner for Public Appointment’s remit.
Members serve an initial term specified within their terms of appointment, usually an initial five years and can be reappointed (dependent on satisfactory appraisal) for a second term allowing up to a maximum of ten years in total.
Other persons, who are not members of the Council, will at the Council’s invitation attend meetings of the Council as advisers or observers.
Deputy-Chair and sub-groups
The Chair shall determine who should deputise for them in their absence, and in the case of any sub-group of the Council, who shall chair that sub-group.
The Council has a standing sub-group – the Research Working Group (RWG), which undertakes the detailed scientific investigations required by the Council’s work, particularly with reference to the prescription of diseases within the Industrial Injuries Disablement Benefit Scheme. The make-up of the RWG is decided by the Chair, in discussion with the RWG Chair.
The Chair will determine the need for other sub-groups as required by the Council’s work programme. In agreement with the Council, they will set their terms of reference, membership and Chair.
Authority
The Council has no executive or operational functions in relation to the Industrial Injuries Disablement Benefit Scheme, which is operated by the DWP and has no authority in relation to individual benefit decisions or appeals.
Conduct and frequency of meetings
Current arrangements are that the full Council meets four times a year, and in addition the RWG also meets four times a year. Further meetings will be arranged if required and as directed by the Chair. Subject to availability of Departmental funding, the Council will conduct a regular open public meeting in different locations of the United Kingdom, offering opportunities for members of the public to question the Council members on matters relating to its advice to Government.
Partnership of the Council
The Private Pensions and Arm’s Length Body Partnership Division within DWP will partner the Council. Partnership will consist of ensuring the Council has the means to carry out its advisory function efficiently and independently and that it operates in line with Government guidance for Non-Departmental Public Bodies and Scientific Advisory Committees.
Partnership of the Council will take place in line with the high level Framework of Principles set out in the Departmental Framework published by the DWP for managing the relationships of the Department with its Arm’s Length Bodies.
The DWP will provide staff to act as the Secretariat for the Council (including experienced scientific support) and provide financial resources for the Council to carry out its business, administered by the Secretariat.
The Department will carry out tailored reviews of the Council as both a Non- Departmental Public Body and a Scientific Advisory Committee, as required by Cabinet Office and Government Office of Science guidance.
These terms of reference will be reviewed, updated and agreed in consultation with the sponsor Department once in each parliament.
Annual report
The Council will publish an annual report, by the end of July each year, setting out its work in the previous year and its forward work programme for the ensuing year.
Publications
Where the Council advises the Secretary of State to make legislative changes to the Industrial Injuries Disablement Benefit Scheme, the Council will prepare a Command Paper to be presented to Parliament by the Secretary of State for Work and Pensions by Command of Her Majesty. Where the Council has carried out a full review of a topic but is not advising the Secretary of State to make legislative changes, the Council will prepare a Position Paper for publication, setting out its conclusions and reasoning. Where there is little evidence to allow the Council to carry out a full review, an Information Note will be published.
The Council shall, with the aid of the Department, provide a website on GOV.UK where minutes of its meetings will be published, copies of its advice to Ministers shall be made available, details of membership, the Council’s remit and other matters and items of information shall be published.
Method of enquiry
The Council’s task is to advise the Secretary of State on the Industrial Injuries Disablement Benefit Scheme. The majority of this work concerns updating the list of Prescribed Diseases and the occupations that cause them for which IIDB can be paid.
Identifying areas of investigation
The Council’s work programme has reactive and proactive elements.
Reactive elements
The Council interprets its reactive role liberally, to include responsiveness to stakeholder questions and the emerging research literature. Its work programme therefore considers requests from many parties, including (but not limited to): The Secretary of State, Members of Parliament, the DWP, medical specialists, trade unions, health and safety professionals and agencies, victim support groups, delegates of public meetings, and Council members themselves. It also takes account of new peer-reviewed research reports, items in the scientific and general press and the decisions of IIDB Upper Tier Tribunals.
This reactive element is an essential ongoing component of the work, valued by stakeholders, and which makes the Council accessible and open to reasonable enquiry, adaptable, and an intelligent user of information.
Proactive elements
The Council employs a range of tools to directly and continuously monitor changing scientific evidence and new topics that may impact on the Industrial Injuries Scheme. These include periodic review of existing Prescribed Diseases and their terms; a watch list of topics from earlier reports; periodic review of IIDB statistics; review of an annual compendium of research abstracts; benchmarking exercises which compare the IIDB list with lists of other schemes; and, when budgetary constraints allow, commissioned reviews of topics of relevance to the work plan.
The Council’s approach
Once an area of investigation has been identified the Council’s approach will typically be to:
- check original sources
- conduct a review of the relevant scientific peer-reviewed literature
- check the reports of major authorities (such as the International Agency for Research on Cancer)
- take evidence from subject experts
- make a public call for evidence and, where appropriate, direct calls for evidence to key informants (e.g., trade unions, health and safety professionals, Health and Safety Executive)
- collate the evidence, summarise it, and formulate a view in the context of the Scheme
- draft an appropriate report, agreed by the RWG and the full Council, setting out the Council’s advice to the Secretary of State for Work and Pensions and to other stakeholders.
Openness and transparency - this requirement to be met in various ways:
- laying and publication of Command Papers in Parliament
- deposit and publication of Position Papers in the Houses of Parliament Libraries
- publication of Information Notes
- deposit and publication of an Annual Report
- publication of the minutes of Council and RWG meetings
- regular public meetings and other stakeholder engagement
- publication of the proceedings of public meetings
- accessibility to stakeholder enquiries
- information published on the IIAC pages on GOV.UK.
Where inquiries are more than trivial and of sufficient public interest there is always an intention to publish and to respond constructively to the original inquirer. Reports shall cite the considered background literature (to allow a transparent audit trail) and offer a glossary where required (to promote understanding).
Appendix C – Members of the Council in 2022/2023
Dr Lesley Rushton Chair OBE BA MSc PhD CStat Hon FFOM
Appointed 1 April 2018, reappointed for a final 2 years from 1 April 2023
Independent scientist
Emeritus Reader in Occupational Epidemiology, Department of Epidemiology and Biostatistics, Imperial College London
Member, UK Committee on Carcinogenicity
Honorary Fellow, Faculty of Occupational Medicine
Professor Raymond Agius MD DM FRCP FRCPE FFOM
Appointed on 1 May 2019 for five years
Independent member with expertise in occupational and environmental medicine and epidemiology
Emeritus Professor of Occupational and Environmental Medicine, University of Manchester
Member, Council of the British Medical Association, representing the Occupational Medicine ‘Branch of Practice’
Co-Chair of the Occupational Medicine Committee (OMC) of the BMA
Medical School Fellow, Royal College of Physicians
Fellow, Royal College of Physicians, Edinburgh
Fellow, Faculty of Occupational Medicine
Professor Kim Burton OBE PhD Hon FFOM
Appointed 1 November 2018 for a five-year term
Independent member with expertise in musculoskeletal disorders
Occupational Health Research Consultant
Professor of Occupational Healthcare, University of Huddersfield
Honorary Fellow, Faculty of Occupational Medicine
Professor John Cherrie BSc PhD CFFOH
Appointed 1 November 2018 for a five-year term
Independent member with expertise in exposure measurement
Professor of Human Health, Heriot Watt University and Principle Scientist, Institute of Occupational Medicine, Edinburgh
Member of the Health and Safety Executive’s Workplace Health Expert Committee
Chartered Fellow, Faculty of the British Occupational Hygiene Society
Keith Corkan BA
Appointed 1 May 2013, reappointed for a final four-year term from 1 May 2019 – completed appointment in April 2023
Independent member with legal expertise
Consultant, Woodfines Solicitors
Member of the Employment Lawyers Association Member of the International Bar
Association Member of the Global Employment Institute
Lesley Francois LLB(Hons) MA LLM
Appointed 1 September 2019 for a five-year term
Independent member with legal expertise
Lawyer, Royds Withy King
Member of Law Society’s Personal Injury Panel
Member of Association of Personal Injury Lawyers accredited with Senior Litigator Status, Occupational Disease Specialist
Status, Asbestos Disease Specialist Status
Dr Richard Heron MB ChB FRCP FFOM SFFMLM
Appointed 3 January 2023 for a five-year term
Representative of employers
Independent Chief Medical Officer
Managing Director, Heron Health Consulting Ltd
Honorary Professorial Fellow, International Business and Health, Department of Medicine, University of Nottingham
Expert Advisor, NHSE/NHSI Health and wellbeing expert advisory group
Co-chair, International Occupational Medicine Society Collaborative
Dr Sally Hemming PhD BSc Sociology MICPD
Appointed 3 January 2023 for a five-year term
Representative of employers
Health & Wellbeing Lead, EY, UKI
Associate wellbeing services, JP Hemming Ltd
Professor Max Henderson MSc PhD MRCP MRCPsych HonFFOM
Appointed 1 November 2018 for a five-year term
Independent member with expertise in psychiatry
Professor, Psychological Medicine & Occupational Psychiatry, University of Leeds
Honorary Fellow, Faculty of Occupational Medicine
Dr Jennifer Hoyle MRCP Edin FRCP
Appointed 1 September 2019 for a five-year term
Independent member with expertise in general and respiratory medicine with an interest in occupational lung disease
Consultant Physician, North Manchester General Hospital
Member, Royal College of Physicians, Edinburgh
Fellow, Royal College of Physicians
Dr Ian Lawson MB BS FFOM FRCP FRSPH
Appointed 1 November 2018, reappointed for a second term of five years, beginning 1 November 2021
Representative of employers, with expertise in hand arm vibration syndrome
Retired Occupational Health Physician, formerly Chief Medical Officer, Rolls-Royce plc
Fellow, Faculty of Occupational Medicine Fellow, Royal College of Physicians
Fellow, Royal Society for Public Health
Professor Damien McElvenny BSc MSc CStat CSci
Appointed 1 December 2021 for a five-year term
Independent member with specialist skills in biostatistics and epidemiology
Principal Epidemiologist, Institute of Occupational Medicine and Senior Research Fellow, Centre for Occupational and Environmental Health, University of Manchester
Member of the Royal Statistical Society
Member of the International Commission on Occupational Health and Secretary of Epidemiology Scientific Committee (EPICOH)
Secretary UK/Ireland Occupational and Environmental Epidemiology Society
Associate Editor, Occupational and Environmental Medicine
Assistant Editor, Occupational Medicine
Karen Mitchell LLB
Appointed on 1 December 2014, reappointed for a second term of five years from 1 December 2017 - completed appointment in November 2022
Representative of employed earners
Retired Legal Officer and Solicitor, National Union of Rail, Maritime and Transport
Steve Mitchell LLB
Appointed 3 January 2023 for a five-year term
Representative of employed earners
Deputy Head of Legal Services, Union of Shop, Distributive and Allied Workers
Douglas Russell BSc (Hons) MSc CMIOSH
Appointed on 1 December 2014, reappointed for a second term for five years from 1 December 2017 - completed appointment in November 2022
Representative of employed earners
National Health and Safety Officer, Union of Shop, Distributive and Allied Workers Chartered Member, Institute of Occupational Safety and Health
Daniel Shears
Appointed 1 September 2018 for a five-year term
Representative of employed earners
National Health, Safety and Environment Director, GMB Trade Union
Member, Health and Safety Executive Industry Advisory Committees including Construction Industry Advisory Committee and Paper and Board Industry Advisory Committee
Member, TUC Union Health and Safety Specialists Committee
Dr Chris Stenton BSc MB BCh BAO FRCP FFOM
Appointed 1 December 2018 for a five-year term
Independent member with expertise in respiratory medicine
Locum Consultant Physician, Royal Victoria Infirmary Fellow, Royal College of Physicians
Fellow, Faculty of Occupational Medicine
Dr Sharon Stevelink BSc PhD MSc
Appointed 3 January 2023 for a five-year term
Independent member with expertise in epidemiology and psychological medicine
NIHR Advanced Fellow, Department of Psychological Medicine, King’s College, London
Senior Lecturer in Epidemiology, Department of Psychological Medicine and King’s Centre for Military Health Research, King’s College, London
Academic member of the Psychological Medicine PhD Sub-Committee, King’s College, London
Chair of the assessment sub-board for MSc in War & Psychiatry, King’s College, London
Associate editorial board member, BMC Psychiatry
Dr Gareth Walters MD FRCP FHEA
Appointed on 1 December 2021 for a five-year term
Independent member with expertise in occupational respiratory medicine and interstitial lung diseases
Honorary Senior Clinical Research Fellow, Occupational Respiratory Medicine, Institute of Applied Health Research, Birmingham University
NHS consultant, Birmingham Chest Clinic
Member, British Thoracic Society (BTS) Clinical Statement Group on occupational asthma
Member, Group of Occupational Respiratory Disease Specialists (GORDS) UK
Dr Andrew White BSc (Hons) PhD CMIOSH AIEMA
Appointed on 1 December 2014, reappointed for a second term of five years from 1 December 2017 - completed appointment in November 2022
Representative of employers
Director of Risk & Assurance, The Pirbright Institute
Chartered Member, Institute of Occupational Safety and Health
Appendix D: IIAC Secretariat, Officials and Observers
IIAC has a secretariat, supplied by the DWP, dedicated to the Council’s requirements. It consists of the Secretary, a Scientific Adviser and an administrative secretary.
Members of the Secretariat
Mr Stuart Whitney: Secretary Mr Ian Chetland: Scientific Adviser Ms Catherine Hegarty: Administrative Secretary
Contact Details
Industrial Injuries Advisory Council
Caxton House
Tothill Street
London
SW1H 9NA
Email: [email protected]
Website: www.gov.uk/iiac
Officials and Observers attending meetings
Officials from the DWP attend Council meetings to give advice and guidance to IIAC on policy matters and the operation of the IIDB Scheme. Representatives from the HSE and the Ministry of Defence attend as observers.
From the DWP
Dr Emily Pikett: Disability Employment and Support Directorate
Dr Mark Allerton: Disability Employment and Support Directorate
Ms Elenor Styles: Disability Employment and Support Directorate
Ms Mandeep Kooner: Disability Employment and Support Directorate
Ms Jo Pears: Disability Employment and Support Directorate
Ms Catriona Hepburn: DWP Legal Services
Mr Lee Pendleton: Benefit Services Directorate
From the HSE
Ms Lucy Darnton: Science, Engineering and Analysis Division
From the MoD
Dr Anne Braidwood: Medical Adviser, Armed Forces Compensation Schemes
Appendix E: Expenditure
The Council does not have a budget of its own. However, DWP provide a small administrative budget of £55,000 to allow the Council to function. This includes:
The IIAC Chair fee of £15,000 per annum, in place from April 2018, and
Fees for members attending IIAC meetings were set from April 2007 as follows:
Full Council meetings: IIAC member £142
Sub-Committee meetings: RWG Chair £182 and RWG member: £142
Travel expenses are also payable in accordance with DWP rates and conditions.
The full Council met four times in 2022-23 and its RWG sub-committee also met four times during the year. To take forward the Council’s reviews of pneumoconiosis and HAVS, some members met online intermittently during the year, and this has been reflected in the fees paid outside of the usual meetings.
Meetings continued to be conducted online, moving to hybrid meetings when it was possible with some members attending in person and others remaining online. Expenses were only claimed by those attending in person.
No public meeting was held during 2022-23.
An overview of expenditure for 2022-23 was as follows:
| Expenditure | Costs |
|---|---|
| Professional fees | £27,474 |
| Expenses | £4,410.54 |
| Printing | £1,127.31 |
| Public Meeting | £0 |
| Research Material | £6.10 |
| Catering | £0 |
| Total | £33,017.95 |
To enable the Council to undertake its heavy workload, the Secretariat also secured additional funding each year to allow the Council to get external reviewers to consider certain scientific information on a topic where the literature is large and provide initial findings.
-
A Command Paper is a Council report that includes a review of the relevant literature and contains recommendations which require changes to legislation (e.g., recommending a disease and/or an exposure be added to the list of prescribed diseases for the purposes of prescription). These papers are laid before Parliament. ↩
-
A Position Paper is a Council report which details a review of a topic that did not result in recommendations requiring legislative changes. These papers are deposited in House libraries. ↩
-
An Information Note is a short summary of an IIAC review which did not result in recommendations requiring legislative changes and where the evidence base is still emerging and may be liable to change, or where there was insufficient evidence to warrant a Position Paper. ↩