Prenatal pertussis vaccination coverage in England from July to September 2022
Updated 20 December 2024
Applies to England

© Crown copyright 2024
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/publications/pertussis-immunisation-in-pregnancy-vaccine-coverage-estimates-in-england-october-2013-to-march-2014/prenatal-pertussis-vaccination-coverage-in-england-from-july-to-september-2022
Main points
This quarterly report evaluates pertussis coverage for women who delivered in the July to September 2022 quarter who were eligible for the prenatal pertussis vaccine from 16 weeks of pregnancy onwards.
The main findings were that:
-
pertussis vaccine coverage in pregnant women for the second quarter of the 2022 to 2023 financial year was 60.2% in July, 59.8 in August and 60.8 in September
-
the mean coverage for the quarter was 60.2%, which was 4.7 percentage points lower than the mean coverage for the same quarter in the 2021 to 2022 financial year
-
the mean coverage for the quarter was also 6.4 percentage points lower than the mean coverage for the same quarter in the 2020 to 2021 financial year
-
this observed decline in coverage has largely been driven by a decrease in London NHS Commissioning Region which had coverage that was 9.0 percentage points lower in September 2022 as compared to September 2020
-
coverage in London has continued to fall behind, now being 29 percentage points lower than the region with the highest coverage (North East and Yorkshire)
Introduction
This report presents pertussis vaccine coverage in pregnant women in England for the period July to September 2022, updating previous data reported for April to June 2022 (1).
Following increased pertussis activity in all age groups, including infants under 3 months of age, and the declaration of a national pertussis outbreak in April 2012 (2), the pertussis vaccine has been offered to pregnant women since 1 October 2012 (3). The prenatal pertussis vaccination programme aims to minimise disease, hospitalisation, and deaths in young infants, through the intrauterine transfer of maternal antibodies, until they can be actively protected by the routine infant programme with the first dose of pertussis vaccine scheduled at 8 weeks of age (4).
In June 2014, the Joint Committee on Vaccination and Immunisation (JCVI) advised it should continue for a further 5 years. In February 2016, the JCVI considered new evidence demonstrating that vaccination earlier in pregnancy would increase opportunities during pregnancy for vaccination, without detrimentally affecting the protection afforded to the infant (5). Based on this, JCVI advised that vaccination could be offered from gestational week 16, although for operational reasons vaccination should ideally be offered from around 20 weeks, on or after the foetal anomaly scan (6).
This advice was implemented from April 2016 as was offering the vaccine through general practice as well as some maternity services. In 2019, following the JCVI recommendation, the prenatal pertussis vaccine became a routine programme in England.
In response to the coronavirus (COVID-19) pandemic, nationwide social distancing measures were initiated from 23 March 2020. To minimise disruptions, guidance to continue routine vaccination programmes with priority given to time sensitive vaccines, such as prenatal pertussis vaccines, were outlined by NHS England at the beginning of the pandemic (7).
In addition, the Royal College of Nursing published guidance on the management of immunisation clinics, and Public Health England (PHE) produced resources promoting immunisations to pregnant women and young families (8).
Methods
GP level pertussis vaccine coverage data is automatically uploaded via participating GP IT suppliers to the ImmForm website each month. ImmForm data is validated and analysed by the UK Health Security Agency (UKHSA) to check data completeness, identify and query any anomalous data and describe epidemiological trends. Since April and May 2016 (implementation date varied by GP IT supplier) the following monthly data has been collected:
- denominator: number of women who delivered in the survey month, excluding miscarriages and stillbirths, regardless of gestational age
- numerator: number of women in the denominator receiving pertussis vaccination between week 16 of pregnancy and delivery
For accurate denominators to be extracted from GP IT systems by the automated survey and precise coverage estimates to be calculated, it is important that the medical records of all women who have given birth have the following fields completed:
- the date of delivery
- the date of receipt of a pertussis-containing vaccine at or after week 16 of pregnancy, regardless of the setting where the vaccine was administered
- where relevant, fields indicating stillbirth or miscarriage
Data is extracted monthly examining the preceding calendar month, but allowance is made for the relevant data items to be recorded, and therefore the extraction is undertaken 3 weeks following the end of the month, that is: April data is extracted on 21 May.
Coverage by former local teams and NHS commissioning regions (based on the 2019 NHS England configurations) is also included in the data tables associated with this report for comparison.
Clinical commissioning groups (CCGs) have been omitted due to changes in NHS geographies over time and the abolition of CCGs from 1 July 2022 with the creation of Integrated Care Boards (ICBs).
Participation and data quality
All GP IT suppliers provided data for the July to September 2022 period. National GP practice participation was at 96.9% (July 2022), 96.1% (August 2022) and 67.1% (September 2022).
Results
Monthly pertussis vaccine coverage ranged across the quarter from 59.8% in August to 60.8% in September, with mean coverage for the quarter at 60.2% (Table 1, Figure 1, see data tables). During this quarter, prenatal pertussis vaccine coverage by ICB ranged from 25.5% (North Central London, August 2022) to 80.9% (Derby and Derbyshire, July 2022) (Table 1).
When compared with data from the 2021 to 2022 financial year, national coverage was 5.2 percentage points lower in July, 5.1 percentage points lower in August and 3.7 percentage points lower in September. Mean coverage for this quarter was 6.4 percentage points lower compared to national coverage reported for the same quarter in the 2020 to 2021 financial year. Coverage between July and September 2022 was the lowest measured since April 2016 when the new IT specification was implemented to capture vaccinations given earlier in pregnancy according to the change in JCVI advice that extended eligibility criteria for the vaccine to be available from 16 weeks gestation (previously 28 weeks)(Figure 1) (9).
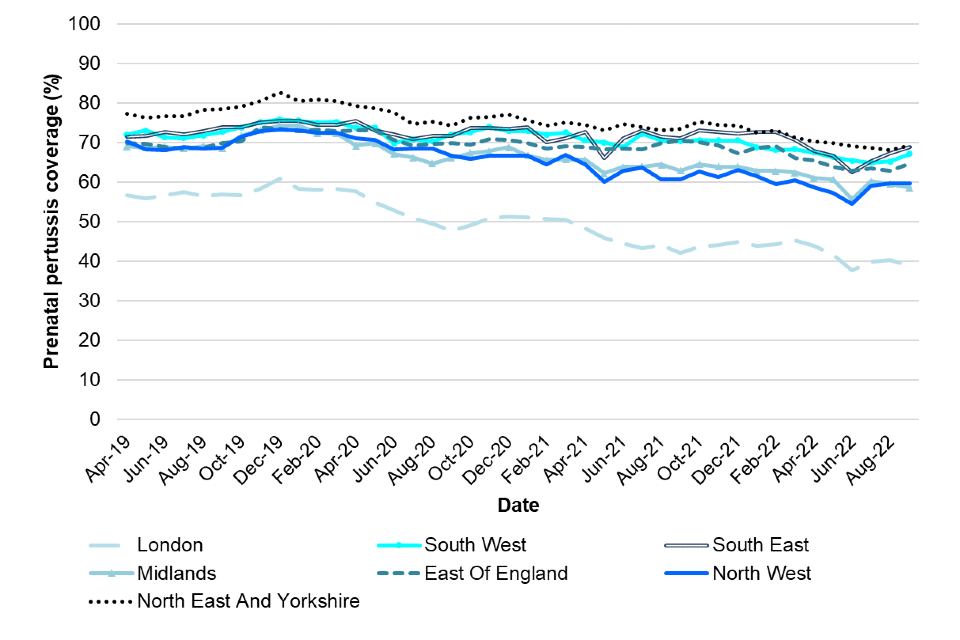
Coverage by former local teams and NHS commissioning regions (based on the 2019 NHS England configurations) are also included in the attached data tables for trend comparisons. In London NHS commissioning region there has been a steep decline in coverage since December 2019. Coverage in London has dropped 22.1 percentage points from December 2019 when coverage was 60.9% to September 2022 when coverage was 38.8% (Figure 2). The disparity between the region with the highest coverage (North East and Yorkshire) and London with the lowest coverage has increased over time, rising from a 20.9 percentage point difference in quarter 2 of 2019 to 2020 to 29 percentage point difference this quarter.
Table 1. Monthly pertussis vaccination coverage (%) in pregnant women by ICB in England, July to September 2022
| ICB code | ICB name | July 2022 | Aug 2022 | Sept 2022 | July to Sept 2022 |
|---|---|---|---|---|---|
| QE1 | Lancashire and South Cumbria | 60.5 | 61.5 | 61.1 | 61.1 |
| QF7 | South Yorkshire | 68.8 | 67.8 | 68.7 | 68.5 |
| QGH | Herefordshire and Worcestershire | 61.7 | 60.7 | 60.9 | 61.1 |
| QH8 | Mid and South Essex | 62.9 | 64.1 | 63.6 | 63.5 |
| QHG | Bedfordshire, Luton, and Milton Keynes | 60.8 | 55.4 | 60.0 | 58.7 |
| QHL | Birmingham and Solihull | 45.6 | 46.0 | 45.8 | 45.8 |
| QHM | North East and North Cumbria | 66.7 | 64.9 | 66.3 | 65.9 |
| QJ2 | Derby and Derbyshire | 80.7 | 75.5 | 72.9 | 76.3 |
| QJG | Suffolk and North East Essex | 62.3 | 66.2 | 67.1 | 65.2 |
| QJK | Devon | 65.2 | 58.9 | 64.7 | 62.9 |
| QJM | Lincolnshire | 62.9 | 63.4 | 63.0 | 63.1 |
| QK1 | Leicester, Leicestershire and Rutland | 57.2 | 58.3 | 61.4 | 59.0 |
| QKK | South East London | 47.4 | 50.1 | 47.1 | 48.3 |
| QKS | Kent and Medway | 62.0 | 63.2 | 66.0 | 63.8 |
| QM7 | Hertfordshire and West Essex | 62.9 | 63.3 | 65.3 | 63.8 |
| QMF | North East London | 33.4 | 33.5 | 33.2 | 33.4 |
| QMJ | North Central London | 27.2 | 25.5 | 26.0 | 26.1 |
| QMM | Norfolk and Waveney | 72.2 | 74.1 | 75.0 | 73.8 |
| QNC | Staffordshire and Stoke-on-Trent | 64.4 | 64.9 | 57.9 | 62.6 |
| QNQ | Frimley | 55.3 | 60.0 | 62.3 | 59.2 |
| QNX | Sussex | 69.0 | 68.4 | 68.9 | 68.8 |
| QOC | Shropshire, Telford and Wrekin | 77.9 | 78.2 | 77.0 | 77.7 |
| QOP | Greater Manchester | 58.1 | 58.1 | 57.0 | 57.8 |
| QOQ | Humber and North Yorkshire | 76.7 | 74.3 | 77.4 | 76.1 |
| QOX | Bath and North East Somerset, Swindon and Wiltshire | 70.9 | 69.8 | 68.9 | 69.9 |
| QPM | Northamptonshire | 53.0 | 52.8 | 52.3 | 52.7 |
| QR1 | Gloucestershire | 62.5 | 58.9 | 65.2 | 62.2 |
| QRL | Hampshire and Isle of Wight | 66.9 | 69.0 | 71.4 | 69.2 |
| QRV | North West London | 40.1 | 40.2 | 35.9 | 38.9 |
| QSL | Somerset | 65.4 | 69.3 | 68.3 | 67.8 |
| QT1 | Nottingham and Nottinghamshire | 65.6 | 68.2 | 67.8 | 67.2 |
| QT6 | Cornwall and Isles of Scilly | 42.9 | 51.5 | 58.5 | 50.8 |
| QU9 | Buckinghamshire, Oxfordshire, and Berkshire West | 68.0 | 70.8 | 71.9 | 70.4 |
| QUA | Black Country | 50.9 | 49.5 | 46.4 | 48.9 |
| QUE | Cambridgeshire and Peterborough | 61.8 | 54.9 | 58.7 | 58.5 |
| QUY | Bristol, North Somerset, and South Gloucestershire | 67.8 | 73.2 | 71.2 | 70.8 |
| QVV | Dorset | 68.6 | 65.6 | 68.1 | 67.4 |
| QWE | South West London | 52.6 | 53.3 | 55.0 | 53.6 |
| QWO | West Yorkshire | 65.1 | 67.3 | 67.4 | 66.6 |
| QWU | Coventry and Warwickshire | 55.2 | 58.9 | 57.2 | 57.3 |
| QXU | Surrey Heartlands | 63.4 | 68.2 | 68.2 | 66.8 |
| QYG | Cheshire and Merseyside | 59.3 | 60.4 | 61.0 | 60.3 |
| Total | 60.2 | 59.8 | 60.8 | 60.2 |
Figure 1. Monthly pertussis vaccination coverage (%) in pregnant women (England), 2016 to 2022
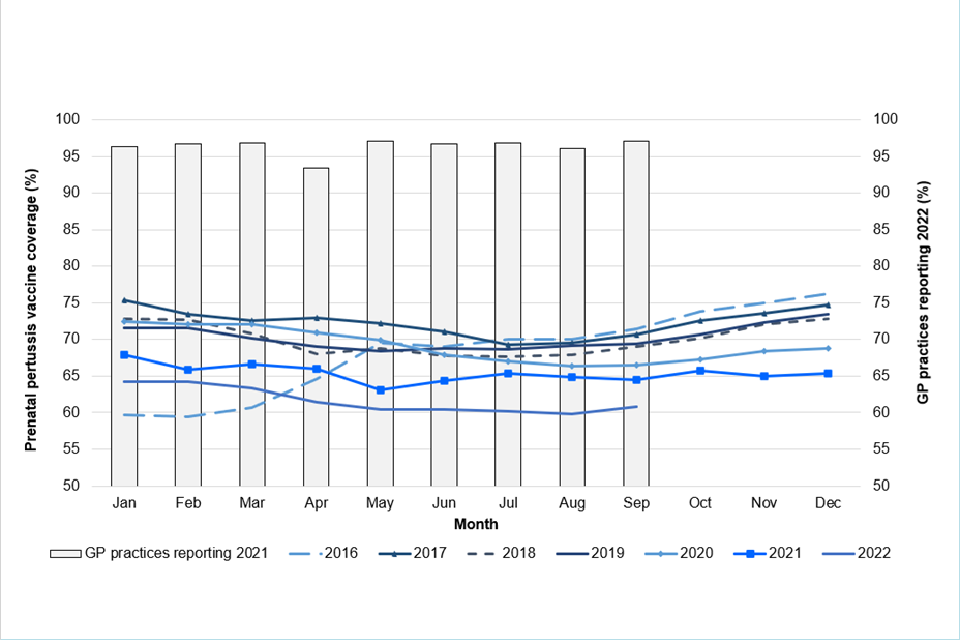
Figure 2. Monthly pertussis vaccination coverage (%) in pregnant women by NHS commissioning region, April 2019 to September 2022
Discussion
The number of confirmed cases in infants under 3 months, who are targeted by the maternal immunisation programme, continues to remain extremely low with no confirmed case between January and March 2022 compared to 0 and 16 cases in the same quarter in 2021 and 2020 respectively (10). It continues to be important to encourage women to be immunised against pertussis at the optimal time during pregnancy in order to protect their babies from birth as levels of disease are likely to increase following the easing of COVID-19 control measures.
This quarterly report evaluates pertussis vaccine coverage for women who delivered in the July to September 2022 quarter. The continuation of the COVID-19 pandemic and its impact on healthcare services has possibly resulted in vaccine coverage this quarter being lower than any previous quarter since April 2016.
Overall, monthly prenatal pertussis vaccine coverage in the second quarter of 2022 to 2023 went from 60.2% in July to 59.8% in August and to 60.8% in September. From July to September 2022, the difference in mean coverage between the highest and lowest ICB was 51.6 percentage points.
Coverage in the London NHS commissioning region has declined substantially since December 2019, falling 22.1 percentage points by September 2022. Sharing learning across the country, including those measures that have been successful in mitigating the impact of social distancing, may help address any gaps in coverage for future cohorts of pregnant women.
Limitations to the data presented in this report may explain the observed variability in coverage at the local level and over time. First, completeness of data is reliant on the recording of delivery dates in the mother’s medical records and a recent study in England suggests that maternity notes regarding pregnancy and delivery are often scanned or archived, rather than coded in an extractable format (11). Furthermore, a comparison of these denominator data with national data on live births (12) indicates that in 2021, this data represented about 71% of the population of pregnant women.
Continued support in the delivery of this important programme has been sought from service providers (GP practices and maternity units), screening and immunisation teams, and health protection teams. Screening and immunisation teams should continue to update service providers on the current epidemiology of the disease and the need to maintain and improve coverage achieved thus far.
If coverage, and ultimately the impact of the programme itself, is to be accurately monitored, it is essential that GPs and practice nurses continue to ensure that vaccination and date of delivery are recorded in the patient’s GP record. In areas that have commissioned maternity units to offer pertussis vaccines in pregnancy, it is important that providers ensure doses of vaccines given to individual women are also communicated to the woman’s GP. Maternity units not offering pertussis vaccines to pregnant women should continue to discuss its importance, make use of available resources (13), and signpost the woman to her GP to receive the vaccine.
GPs, practice nurses, obstetricians, and midwives should continue to encourage pregnant women to receive the pertussis vaccine, ideally, between weeks 20 and 32 of their pregnancy (but up to term) to optimise protection for their babies from birth (6).
References
1. UKHSA (2022). Pertussis vaccination programme for pregnant women update: vaccine coverage in England, April to June 2022. Health Protection Report: volume 16, number 12
2. PHE (2012). A level 3 incident is the third of 5 levels of alert under the PHE’s Incident Reporting and Information System (IERP) according to which public health threats are classified and information flow to the relevant outbreak control team is coordinated. A level 3 incident is defined as one where the public health impact is significant across regional boundaries or nationally. An IERP level 3 incident was declared in April 2012 in response to the ongoing increased pertussis activity.
3. PHE (2012). Pregnant women to be offered whooping cough vaccination
4. PHE (2018). ‘Complete routine immunisation schedule’
5. JCVI (2014). Minute of the meeting on 4 June 2014
6. Eberhardt CS, Blanchard-Rohner G, Lemaitre B, Boukrid M, Combescure C, Othenin-Girard V and others (2016). ‘Maternal immunization earlier in pregnancy maximizes antibody transfer and expected infant seropositivity against pertussis’ Clinical Infectious Diseases: volume 62, pages 829 to 836
7. JCVI (2016). Minute of the meeting on 3 February 2016
8. PHE (2016). The Green Book, chapter 24: Pertussis
9. JCVI (2019). Minute of the meeting on 5 June 2019
10. NHS England (2020). Preparedness letter for general practice: 14 April 2020
11. Royal College of Nursing (2020). Immunisation
12. PHE (2020). Vaccine update: World Immunisation Week
13. PHE (2016). Pertussis vaccination programme for pregnant women: vaccine coverage estimates in England, April 2016 to September 2016
14. UKHSA (2022). ‘Laboratory confirmed cases of pertussis in England: October to December 2021.’ Health Protection Report: volume 16 number 6
15. Llamas A, Amirthalingam G, Andrews N, and Edelstein M (2020). ‘Delivering prenatal pertussis vaccine through maternity services in England: what is the impact on vaccine coverage?’ Vaccine: volume 38, issue 33, pages 5,332 to 5,336
16. Office for National Statistics (2022). Provisional births in England and Wales
17. PHE (2017). Pregnancy: How to help protect you and your baby