Musculoskeletal diseases profile: short commentary, December 2018
Published 4 December 2018

© Crown copyright 2018
This publication is licensed under the terms of the Open Government Licence v3.0 except where otherwise stated. To view this licence, visit nationalarchives.gov.uk/doc/open-government-licence/version/3 or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or email: [email protected].
Where we have identified any third party copyright information you will need to obtain permission from the copyright holders concerned.
This publication is available at https://www.gov.uk/government/statistics/musculoskeletal-diseases-profile-december-2018-update/musculoskeletal-diseases-profile-short-commentary-december-2018
New in this update
In this update, one new indicator has been added to the musculoskeletal (MSK) diseases profile and 3 indicators have been updated with new data points.
The following indicator is new to the profile:
- percentage reporting at least 2 long term conditions, at least one of which is MSK related
The following indicators have been updated with new data points:
- percentage reporting a long term MSK problem
- rheumatoid arthritis: Quality and Outcomes Framework (QOF) prevalence (aged 16 and over)
- osteoporosis: QOF prevalence (aged 50 and over)
Summary
Percentage reporting a long term MSK problem, GP Patient Survey, 2017 to 2018
In 2017 to 2018, 17.0% of people in England reported a long term MSK problem. This varied between upper tier local authorities; Wandsworth had the lowest level at 8.6% and Hartlepool the highest at 26.9%.
The percentage of people reporting a long term MSK problem significantly increased with age, with 2.8% of 18 to 24 years olds reporting an MSK problem compared with 43.7% in the 85 years and over category. Women reported a significantly higher prevalence of MSK problems than men (19.0% compared with 14.9%).
Prevalence of long term MSK problems varied by ethnicity, with the highest prevalence (21.3%) in those who were Irish, compared to the lowest prevalence (6.0%) in the Chinese ethnic group. Rates also varied by working status and were highest in the ‘other inactive’ working status group (43.4%) and lowest in those who were in full-time education (2.6%).
Percentage reporting at least 2 long-term conditions, at least one of which is MSK related, GP Patient Survey, 2017 to 2018
The percentage of people who reported at least 2 long term conditions, at least one of which is MSK related was 12.1% for 2017 to 2018. Prevalence varied significantly by age; those in the younger age bands had a lower prevalence of MSK co-morbidity. In the 18 to 24 years age band the prevalence was 1.6% compared with 39.3% in the 85 years and over age band. Women reported a significantly higher prevalence of MSK co-morbidity than men (13.5% compared with 10.6%).
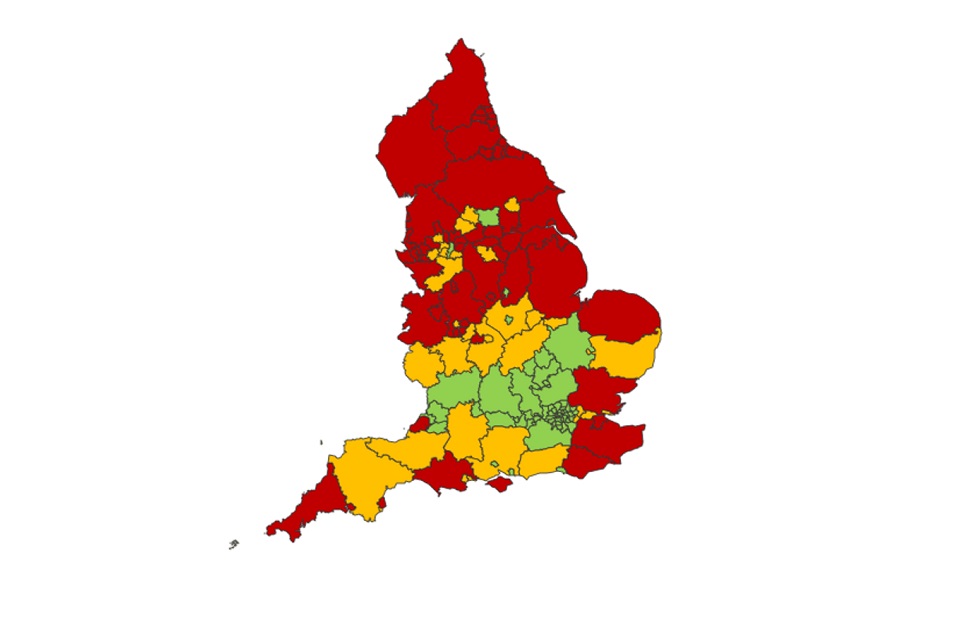
Prevalence of MSK co-morbidity was higher in the north compared with the south, 16.7% of people reported a long term MSK problem in the North East compared to 8.7% in London (Figure 1).
Prevalence varied by working status where the lowest prevalence was in those in fulltime education (1.4%) and highest in the retired group (27.4%). Rates varied between full time work (4.4%) and part time work (7.3%). Rates also varied by ethnicity, where the highest prevalence was in those who were Irish (16.2%) and lowest in the Chinese group (3.0%). There were also differences by deprivation decile.
Data for this indicator has been added from 2014 to 2015 up to 2017 to 2018. It shows an increase from the first data point, where prevalence of MSK co-morbidity was 11.4% to 12.1% in 2017 to 2018.
Figure 1: Percentage who have at least 2 long term conditions, at least one of which is MSK related, by upper tier local authorities in England, 2017 to 2018
Rheumatoid Arthritis: QOF prevalence (aged 16 and over), 2017 to 2018
In 2017 to 2018, the prevalence of rheumatoid arthritis (aged 16 and over) in the Quality and Outcomes Framework (QOF) was 0.7%.This was similar to the value in 2016 to 2017.
At upper tier local authority level, in 2017 to 2018 the prevalence varied from 1.2% in Gateshead to 0.4% in Kensington and Chelsea. At upper tier level, the prevalence was the same at the most deprived decile and least deprived decile (0.7%).
Osteoporosis: QOF prevalence (aged 50 and over), 2017 to 2018
The prevalence of osteoporosis (aged 50 and over) in 2017 to 2018 increased from the previous year (0.5%) to 0.6%, as measured by the Quality and Outcomes Framework (QOF). In 2017 to 2018, this varied between upper tier local authorities from 1.4% in Bristol to 0.2% in Newham.
The prevalence of osteoporosis was higher in the least deprived decile (0.8%) than in the most deprived decile (0.6%) at upper tier level. This was also the case at lower tier level.
Background and further information
The musculoskeletal diseases profile aims to provide meaningful data, on a single platform, to enable the commissioning of high value musculoskeletal services. Musculoskeletal data is essential for understanding the health needs of local populations, the number of people accessing services, the cost of services and the outcomes services deliver.
Indicators should not generally be used in isolation but are best looked at in combination to produce an overall picture of the local situation. By using these in conjunction with other locally available data, organisations can undertake a ‘deep dive’ into areas of interest. This more structured approach should be used to uncover the deeper reasons underlying variation, identify opportunities for improvement and support the necessary work to deliver high-value services for people with musculoskeletal conditions.
Responsible statistician, product lead: Alice Stonham
For queries relating to this publication, please contact: [email protected]