West Nile virus: epidemiology, diagnosis and prevention
Clinical advice on West Nile virus including symptoms, diagnosis and epidemiology.
West Nile virus (WNV) belongs to a group of viruses known as arboviruses which are transmitted by arthropods. WNV belongs to the genus Flavivirus within the Flaviviridae family, along with other viruses such as dengue and yellow fever.
Although the reservoir of WNV is birds, the virus can be transmitted to humans and horses via mosquitoes, mainly Culex species.
Epidemiology
WNV was first detected in the West Nile district of Uganda in 1937 and the first large outbreak in Europe occurred in Romania in 1996. Cases have been identified in several countries across Europe including France, Italy, Portugal and Spain. See weekly updates on cases in Europe.
In 1999, WNV spread to North America and has subsequently been detected there in all states except Alaska and Hawaii. Between 1999 and 2016, there were more than 45,000 cases and over 2,000 deaths. See CDC maps and data.
Risk to the UK
To date, locally acquired WNV infection has not been reported in the UK, although there have been occasional cases of travel-associated infection. Historically, therefore, the main risk of WNV for UK residents has been for those travelling abroad.
However, in 2010 the mosquito Culex modestus was detected in the UK for the first time since 1944. This mosquito species is the principle bridge vector (responsible for transmission between birds, horses and humans) for WNV in Southern Europe. This finding may increase the risk of WNV being transmitted in the UK.
The map below shows where these mosquitoes have been detected. Mosquito surveillance activities indicate that they are now established on the land adjoining either side of the Thames estuary. Surveillance of other parts of the UK is ongoing but to date C. modestus has not been detected elsewhere in England.
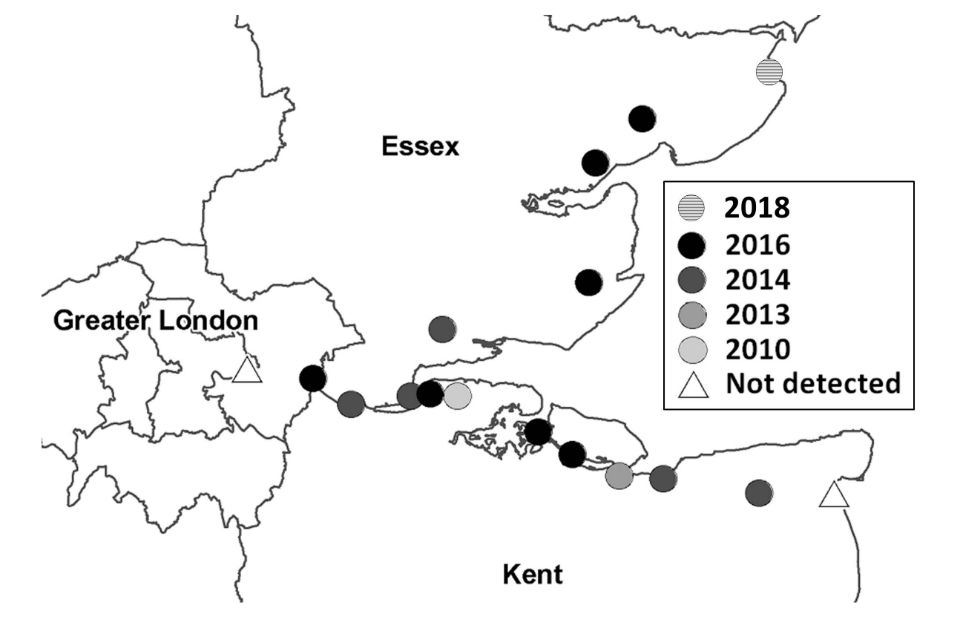
Map showing known distribution of Culex modestus mosquitoes in south-east England.
West Nile virus infection
Most infections in humans are asymptomatic (80%). In those who develop symptoms, patients mainly present with a mild flu-like febrile illness, sometimes called West Nile fever. However, a small proportion (less than 1%) of those infected will develop more severe disease – usually encephalitis, meningitis or meningo-encephalitis.
People over the age of 50 are more likely to develop severe disease and about 10% of neurological infections are fatal.
Symptoms
The incubation period is typically 2 to 6 days, but ranges from 2 to 14 days, and up to 21 days in immunocompromised people. While most infected people are asymptomatic, the majority of clinical cases are mild and present with a sudden onset of influenza-like illness (fever, headache, myalgia). This may include lymphadenopathy and a maculopapular or morbilliform rash on the neck, trunk, arms or leg. Most uncomplicated infections resolve in 3 to 6 days.
Less than 1% (about 1/150) of infected individuals develop neuroinvasive disease which typically presents as meningitis, encephalitis or acute flaccid paralysis. Symptoms include high fever, neck stiffness, stupor, disorientation, tremors, convulsions, severe muscle weakness, paralysis and coma. Ataxia, cranial nerve abnormalities, myelitis, eye pain, polyradiculitis and seizures have also been reported.
Those aged over 50 or with underlying medical conditions (such as cancer, diabetes, hypertension and kidney disease) are at greatest risk of severe disease. The case fatality rate is highest in patients aged over 70.
Laboratory diagnosis
WNV infection should be considered as a differential diagnosis in any person with a febrile or acute neurological illness, particularly with a travel history to southern and eastern Europe, Africa or North America. It should also be considered for those living in or visiting the land adjoining the Thames estuary (North Kent and Essex coastline). See map above.
Testing can be arranged with the PHE Rare and Imported Pathogens Laboratory. If WNV is suspected, the referring clinician should contact a clinician at RIPL to discuss the case.
Rare and imported pathogens laboratory (RIPL)
UK Health Security Agency
Manor Farm Road
Porton Down
Wiltshire
SP4 0JG
Email [email protected]
Telephone 01980 612348 (available 9am to 5pm, Monday to Friday)
DX address DX 6930400, Salisbury 92 SP
WNV is a notifiable organism and should be notified to Public Health England if detected.
Treatment and prevention
No vaccine or specific antiviral treatment is available.
To reduce the risk of WNV infection, travellers to risk areas should practise mosquito bite avoidance measures.
Further advice for travellers is available from the National Travel Health Network and Centre (NaTHNaC) website.
Over the counter pain relievers can be used to reduce fever and relieve severe symptoms. In severe cases, patients often need to be hospitalised to receive supportive treatment such as IV fluids, pain medication and nursing care.
WNV in animals
See information about WNV disease in animals.
Mosquito surveillance
Updates to this page
Published 1 April 2013Last updated 20 August 2018 + show all updates
-
New versions of maps added to page reflecting 2018 data.
-
Added links to NHS Choices West Nile virus page and PHE mosquito surveillance page.
-
First published.